Category: Parkinson’s Disease: Clinical Trials
Objective: This post-hoc analysis of the EPSILON study evaluated whether levodopa dose (<400mg/day vs. ≥400mg/day) and opicapone (OPC) timing (at double-blind [DB] or open-label extension [OLE] baseline) influence the risk of motor complications (MCs) over 1.5 years.
Background: Levodopa is the most effective treatment for Parkinson’s disease (PD), but higher doses increase the risk of MCs, namely wearing-off and dyskinesia [1]. The 24-week, DB EPSILON study showed that adding OPC improved motor impairment in early PD patients without increasing MCs [2]. After the 1-year OLE, OPC provided sustained motor improvement without an increased risk for motor complications.
Method: EPSILON was a randomised, DB, placebo-controlled study, followed by a 1-year OLE. In the DB phase, levodopa-treated PD patients without MCs received OPC 50 mg or placebo. In the OLE phase, all received OPC 50 mg with a key endpoint being the change in MDS-UPDRS-IV scores (motor complications). This exploratory analysis compared time to motor complications, and the subitems dyskinesia (item 4.1) and OFFs (item 4.3) over 1.5 years in patients started with OPC (OPC-OPC) and those who switched from placebo (PLC-OPC), stratified by nominal levodopa dose (<400mg/day vs. ≥400mg/day) at the time of onset of motor complications (event). Data were analysed using Kaplan–Meier survival curves with log-rank tests.
Results: A higher levodopa dose (≥400mg/day) showed a trend for increased risk of MCs, particularly in patients who started OPC later. The proportions of patients without motor complications were 81.9% (<400mg/day) and 79.0% (≥400mg/day) in the OPC-OPC group, versus 73.3% (<400mg/day) and 66.7% (≥400mg/day) in the PLC-OPC group (p=0.04) [Figure 1a]. The proportion of patients without dyskinesia followed a similar trend (p=0.06), while the proportion without OFFs was slightly higher in the OPC-OPC group but independent of baseline levodopa dose (p=0.7) [Figure 1b, c].
Conclusion: Although most patients remain free of MCs with early OPC use, this exploratory analysis reports a trend towards higher risk of MC in those with higher levodopa doses (≥400mg/day) who started OPC later. While further research is needed, early OPC introduction may promote motor stability even in patients on higher levodopa doses.
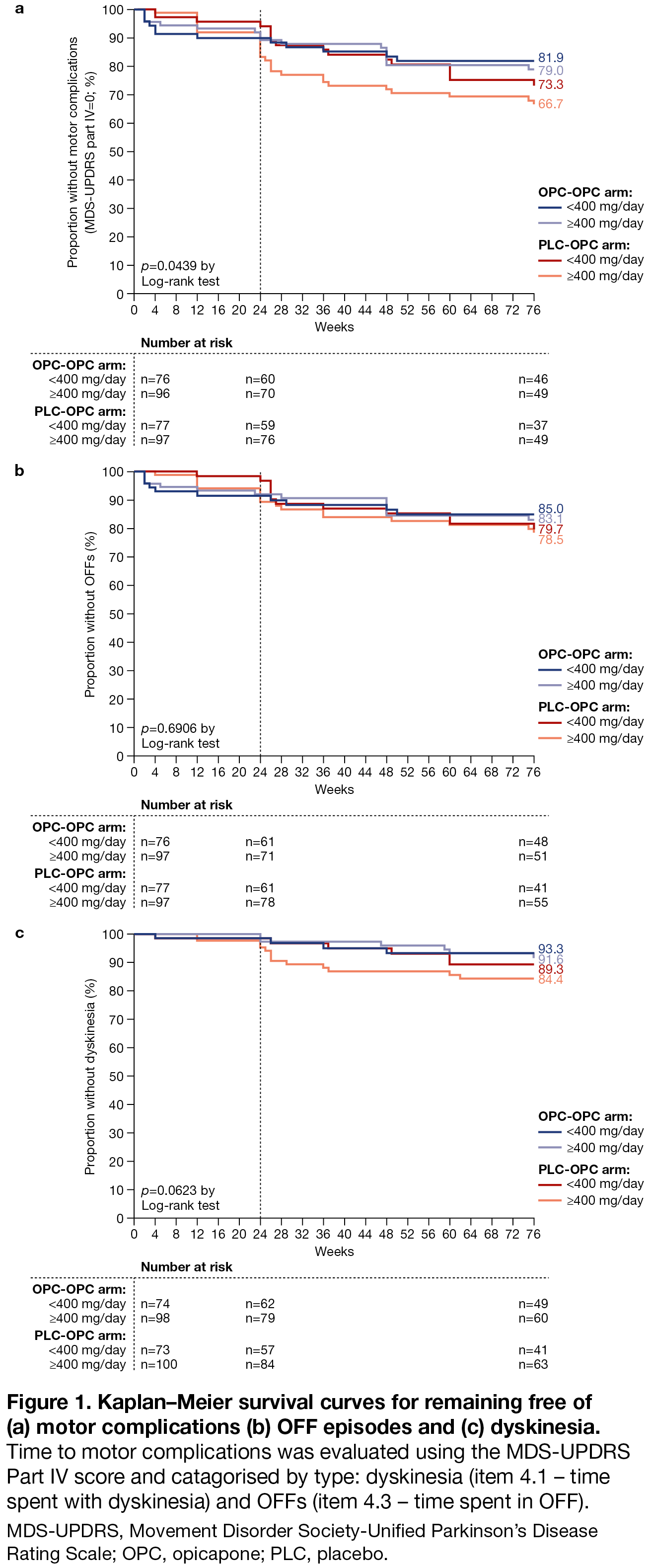
Figure 1
References: 1. Olanow WC, et al. Mov Disord. 2013;28(8):1064-71.
2. Ferreira JJ, et al. Eur J Neurol. 2025;32(1):e16420.
To cite this abstract in AMA style:
J. Ferreira, O. Rascol, F. Stocchi, A. Antonini, H. Brigas, J. Moreira, JF. Rocha, M. Fonseca, D. Ramos, J. Holenz, W. Poewe. Risk of Motor Complications in Early Parkinson’s Disease Patients Treated with Opicapone in the EPSILON study: Effect of Levodopa Dose [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/risk-of-motor-complications-in-early-parkinsons-disease-patients-treated-with-opicapone-in-the-epsilon-study-effect-of-levodopa-dose/. Accessed April 10, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/risk-of-motor-complications-in-early-parkinsons-disease-patients-treated-with-opicapone-in-the-epsilon-study-effect-of-levodopa-dose/