Category: Myoclonus/Tics/Stereotypies
Objective: In order to determine fixed-site and fixed-dose BoNT injections for HFS were easy to administer, safe, efficacious, well-tolerated, and practical this study aims to provide an injection paradigm.
Background: It has been demonstrated that hemifacial spasm (HFS) can be safely and effectively treated with botulinum toxin (BoNT). However, there is ongoing debate over the dosage, duration, and injection techniques of each treatment.
Method: OnabotulinumtoxinA was injected into 4 distinct locations at orbital sections of the orbicular oculi muscle on the affected side of the face at a dose of 5 U/0.1 milliliters. Primary effectiveness was evaluated at weeks 4, 8, and 12 following injection using the Thai version of the Hemifacial Spasm Questionnaire-30 (Thai HFS-30). Secondary efficacy was measured using the 6-point disability rating scale at weeks 2, 4, 8, and 12 and the self-assessment of symptom improvement (0–100%) at week 4. The study’s sample size was determined to be at least 33 participants with a 20% dropout rate. A p-value of less than 0.05 considered statistically significant.
Results: 49 patients with hemifacial spasms. After 2, 4, 8, and 12 weeks of treatment, the mean total Thai HFS-30 score dropped significantly from 48.88 at baseline to 9.63, 7.71, 9.41, and 35.06. Every Thai HFS-30 domain’s analysis results revealed a similar trend. At weeks 0, 2, 4, 8, and 12 after injections, there was a statistically significant decrease (p < 0.001) in the mean 6-point disability rating scale. 71% of patients had improved by more than 80%, 20% by 60–80%, and only 8% by 20–60%, according to the fourth week’s self-assessment of symptom improvement. Furthermore, no patient reported improvement of less than 20%. Two patients experienced localized bruising at the injection sites, which went away completely in three days, and eight patients complained of eyebrow asymmetry as adverse effects following the treatment, which affected ten patients (20.41%). It is noteworthy that no reports of mouth drooping or ptosis were made.
Conclusion: Significant, long-lasting improvements over baseline were observed in a number of symptom and quality of life measures following onabotulinumtoxinA injections administered at particular locations and dosages. Many hemifacial spasm patients may benefit from this safe, useful, and efficient injection procedure, even with little prior experience.
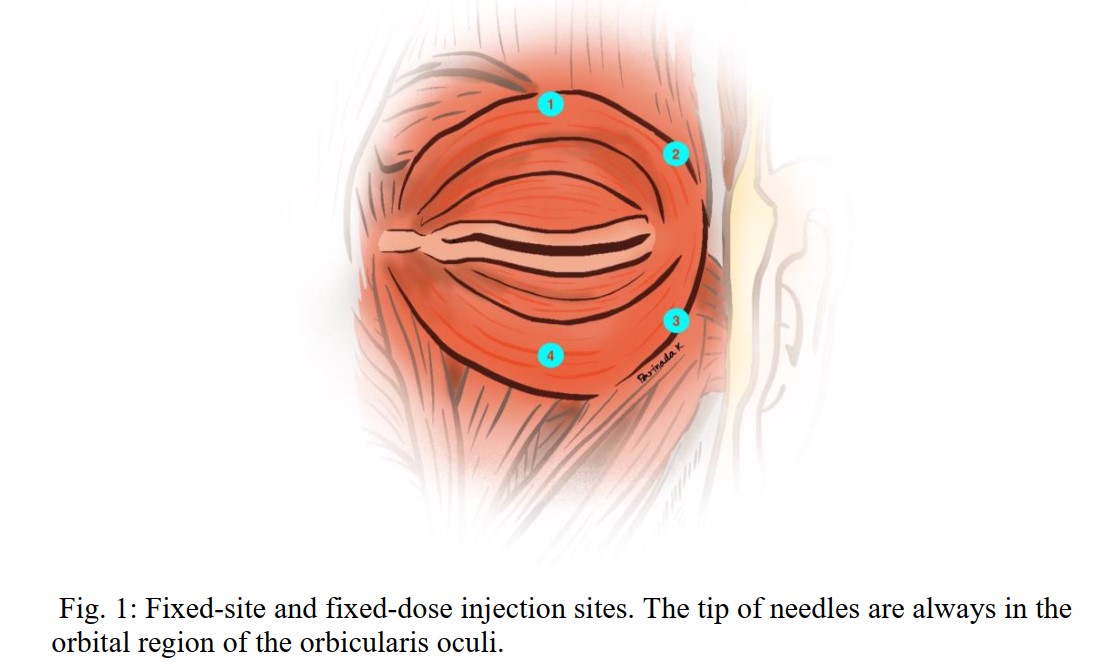
Figure1
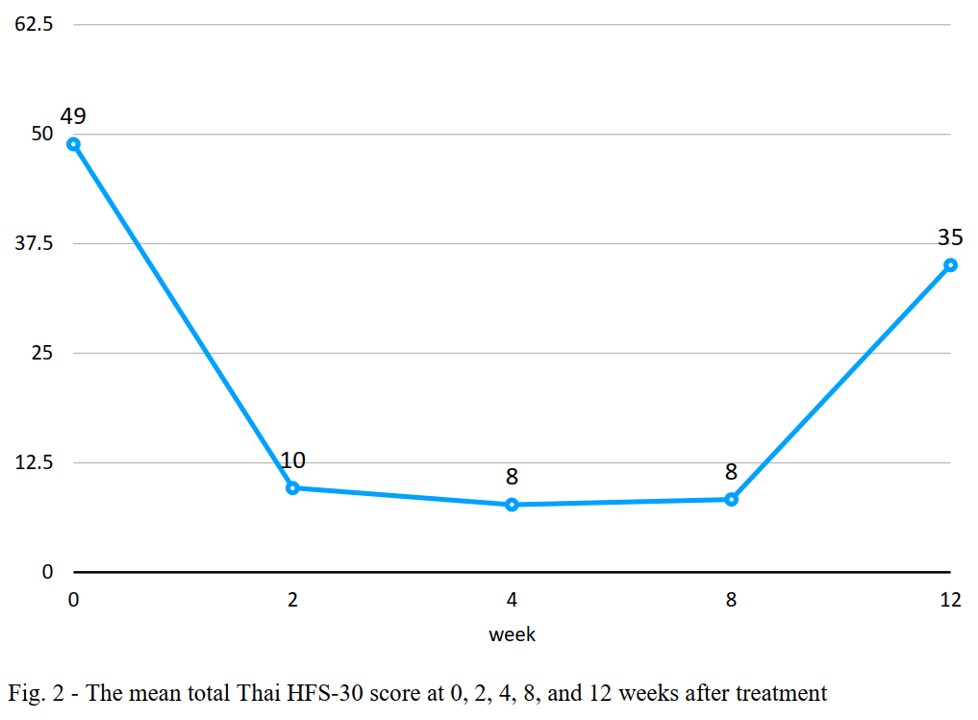
Figure2
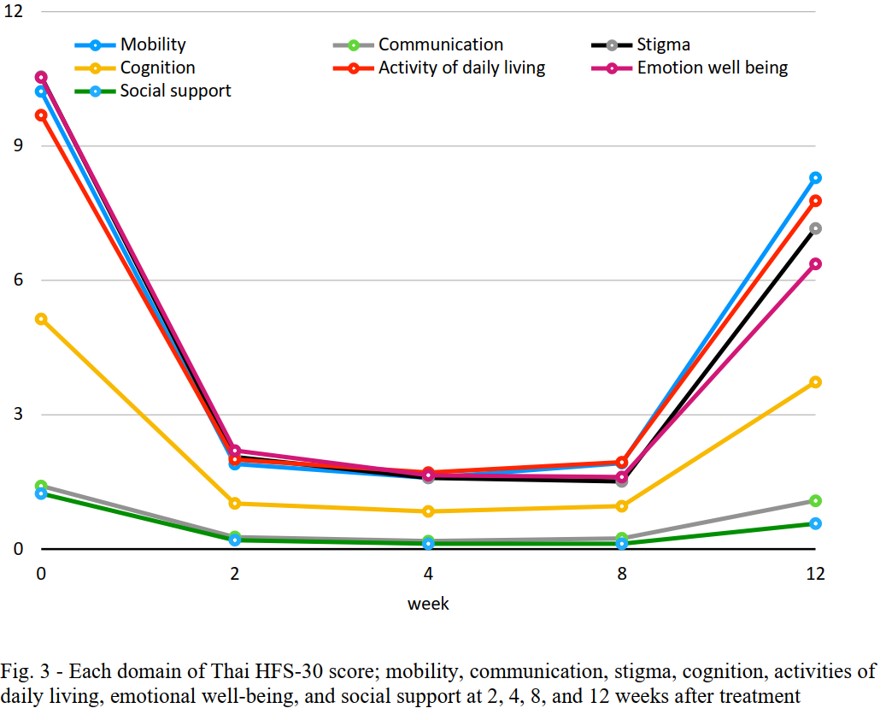
Figure3
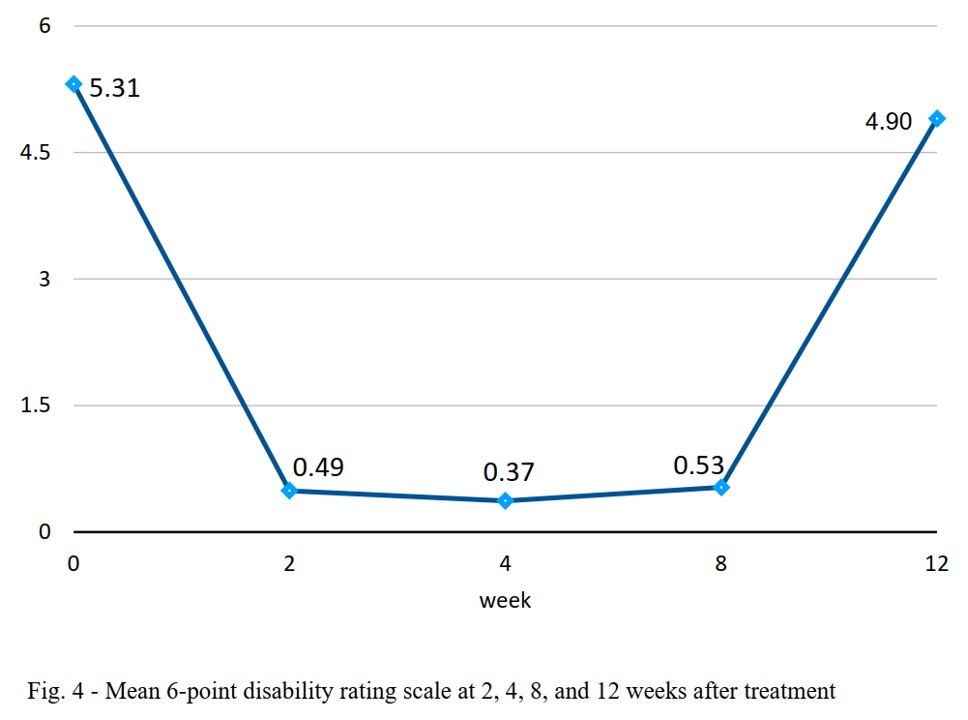
Figure4

Figure5
References: 1. Lu AY, Yeung JT, Gerrard JL, Michaelides EM, Sekula RF, Jr., Bulsara KR. Hemifacial spasm and neurovascular compression. ScientificWorldJournal. 2014;2014:349319.
2. Xiang G, Sui M, Jiang N, Luo R, Xia J, Wei X, et al. The progress in epidemiological, diagnosis and treatment of primary hemifacial spasm. Heliyon. 2024;10(19):e38600.
3. Rosenstengel C, Matthes M, Baldauf J, Fleck S, Schroeder H. Hemifacial spasm: conservative and surgical treatment options. Dtsch Arztebl Int. 2012;109(41):667-73.
4. Tambasco N, Filidei M, Nigro P, Parnetti L, Simoni S. Botulinum Toxin for the Treatment of Hemifacial Spasm: An Update on Clinical Studies. Toxins (Basel). 2021;13(12).
5. Cillino S, Raimondi G, Guepratte N, Damiani S, Cillino M, Di Pace F, et al. Long-term efficacy of botulinum toxin A for treatment of blepharospasm, hemifacial spasm, and spastic entropion: a multicentre study using two drug-dose escalation indexes. Eye (Lond). 2010;24(4):600-7.
6. Jitpimolmard S, Tiamkao S, Laopaiboon M. Long term results of botulinum toxin type A (Dysport) in the treatment of hemifacial spasm: a report of 175 cases. J Neurol Neurosurg Psychiatry. 1998;64(6):751-7.
7. Lolekha P, Choolam A, Kulkantrakorn K. A comparative crossover study on the treatment of hemifacial spasm and blepharospasm: preseptal and pretarsal botulinum toxin injection techniques. Neurol Sci. 2017;38(11):2031-6.
8. Colakoglu BD, Cakmur R, Uzunel F. Is it always necessary to apply botulinum toxin into the lower facial muscles in hemifacial spasm?: a randomized, single-blind, crossover trial. Eur Neurol. 2011;65(5):286-90.
9. Jitpimolmard S, Thinkhamrop B, Tiamkao S, Arunpongpaisal S, Arayavichanon P, Kosuwan W, et al. A Double-Blind, Placebo-Controlled Study of Appropriate Site of Botulinum Toxin Therapy in Hemifacial Spasm. Adv Ther. 2022;39(5):2025-34.
10. Setthawatcharawanich S, Aui-aree N, Limapichart K, Satirapunya P, Phabphal K. The validation of the disease-specific questionnaire for health-related quality of life in Thai patients with hemifacial spasm. J Med Assoc Thai. 2008;91(11):1691-7.
11. Lee JA, Jo KW, Kong DS, Park K. Using the new clinical grading scale for quantification of the severity of hemifacial spasm: correlations with a quality of life scale. Stereotact Funct Neurosurg. 2012;90(1):16-9.
12. Au WL, Tan LC, Tan AK. Hemifacial spasm in Singapore: clinical characteristics and patients ‘ perceptions. Ann Acad Med Singap. 2004;33(3):324-8.
13. Maytharakcheep S, Bhidayasiri R. Botulinum toxin treatment for hemifacial spasm: harmonising neurological and aesthetic outcomes. J Neural Transm (Vienna). 2024.
To cite this abstract in AMA style:
K. Fungpunyaroj, P. Chairangsaris. Simple and Effective OnabotulinumtoxinA Injection Technique for Hemifacial Spasm [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/simple-and-effective-onabotulinumtoxina-injection-technique-for-hemifacial-spasm/. Accessed April 7, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/simple-and-effective-onabotulinumtoxina-injection-technique-for-hemifacial-spasm/