Category: Ataxia
Objective: To report the first Indian patient with SCA 49 who presented in the second decade and to expand the clinical phenotype to include dystonic tremor and bradykinesia.
Background: Variants in SAMD9L gene are known to cause Ataxia-Pancytopenia syndrome (ATXPC) and recently, the ataxia with hyperreflexia phenotype (without pancytopenia) of SAMD9L variation has been assigned as spinocerebellar ataxia 49 (SCA49). It likely results from mitochondrial dysregulation with impaired lysosomal/autophagy pathway
Method: A 23-year-old euthyroid female born to non-consanguineous parentage and no family history presented with progressive gait imbalance, dysarthria, writing problems, and jerky tremulousness of the neck, developing over a period of five years. On examination, cognitive evaluation was normal; slow and hypermetric saccades with bilateral horizontal gaze-evoked nystagmus observed. Visual acuity, color vision and fundus examination were normal. Sensory and motor examination were normal. Bilaterally impaired finger-nose test, dysdiadochokinesia, impaired heel-knee-shin test, and ataxic gait noted. A dystonic neck tremor was discerned with right torticollis and left laterocollis. Geste antagoniste in the form of touching the left side of the neck was also noticed. She had bilateral bradykinesia. Deep tendon reflexes were brisk. The plantar response was flexor.
Results: Routine blood investigations including serum alpha fetoprotein were normal. Autonomic function test and nerve conduction studies were normal. MRI brain showed prominent vermian and cerebellar atrophy (Figure 1). Whole exome sequencing revealed the presence of a novel heterozygous frameshift deletion variation, SAMD9L(NM_152703.5):c.2494del; p.Thr832HisfsTer3 (allele depth, wild/mutant: 30/40). The variant was classified as likely pathogenic (PVS1 and PM2 criteria). Segregation analysis was not performed as the family refused further testing. The patient was offered botulinum toxin therapy for cervical dystonia, which she refused. She was initiated on Trihexyphenidyl (dose 4 mg), and gait/balance rehabilitation. The patient reported no improvement at six months of follow up.
Conclusion: We report the first Indian patient with SCA49 due to a novel frameshift deletion variant, and the twelfth case worldwide. Our case expands the clinical phenotype of SCA49 to include dystonia and parkinsonism.
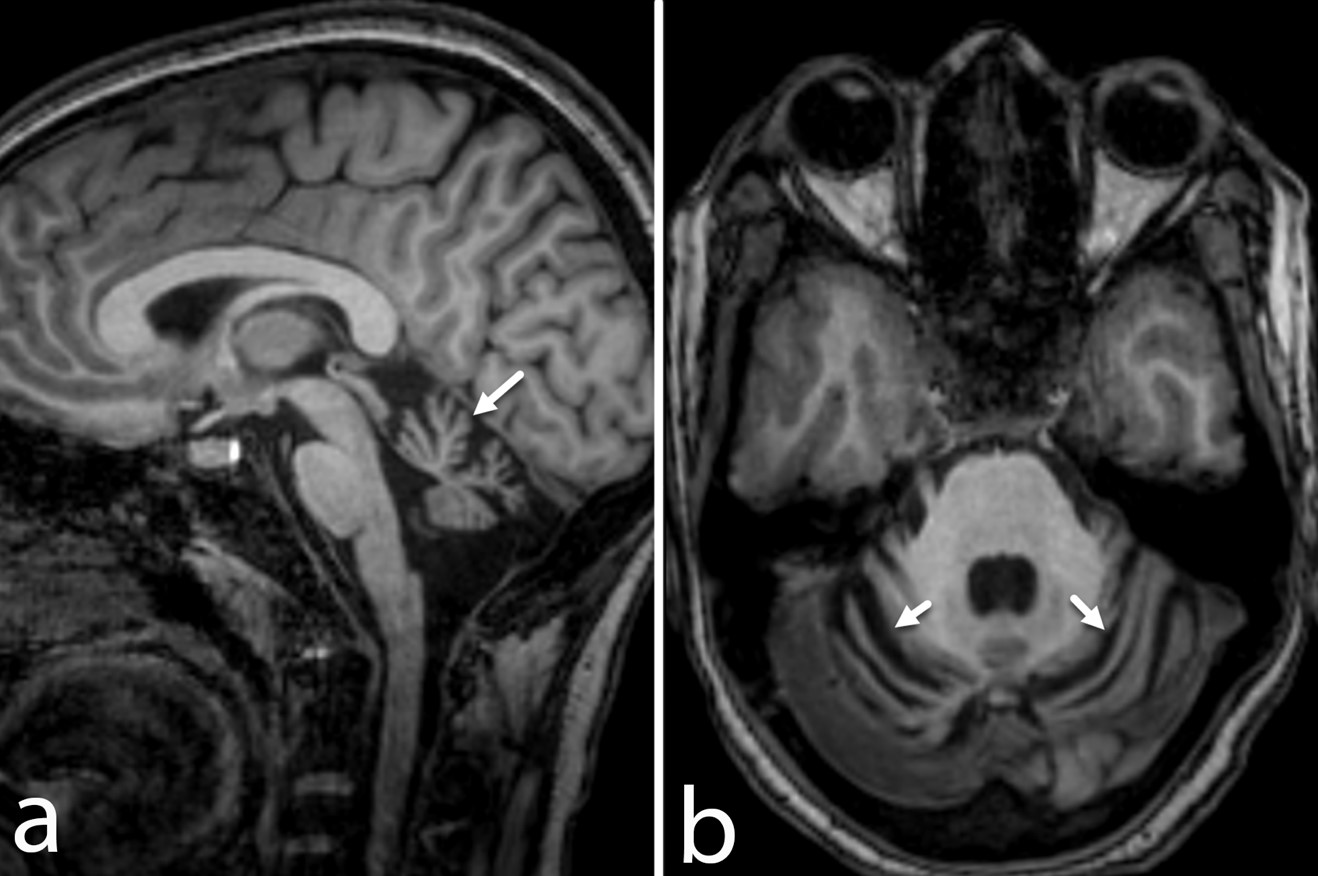
MRI Brain showing cerebellar atrophy
To cite this abstract in AMA style:
P. Saroja Bylappa, D. Garg, P. Sharma, M. Faruq, A. Agarwal, A. Garg, A. Srivastava. Spinocerebellar Ataxia Type 49 presenting with Early onset Dystonia-Ataxia in an Indian Female [abstract]. Mov Disord. 2024; 39 (suppl 1). https://www.mdsabstracts.org/abstract/spinocerebellar-ataxia-type-49-presenting-with-early-onset-dystonia-ataxia-in-an-indian-female/. Accessed July 14, 2026.« Back to 2024 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/spinocerebellar-ataxia-type-49-presenting-with-early-onset-dystonia-ataxia-in-an-indian-female/