Category: Dystonia: Genetics
Objective: To evaluate whether these symptoms, previously categorized as dystonic, might represent manifestations of a temperature-sensitive channelopathy with myotonic features [1].
Background: We report two cases of childhood-onset sporadic paroxysmal exercise-induced dystonia (PED). Case 1 had a mild phenotype, while Case 2 was complicated by seizures and encephalopathy. Despite these differences, both cases shared the same pathogenic variant (G1306) in the voltage-dependent skeletal muscle sodium channel alpha subunit (SCN4A).
Method: Clinical evaluation and whole-exome sequencing (WES) were performed in two unrelated female patients. Case 1: A 21-year-old woman with PED since age 3, initially manifesting during ballet activities. Symptoms began as hand cramping during fine motor tasks, progressing to jaw involvement and mild dysphagia, with exacerbation during exercise. Case 2: A 6-year-old female with more severe PED starting at 12 months, presenting with eyelid ptosis and leg posturing during exercise, dysarthria, and dysphonia. Her condition was complicated by frequent seizures (10/day), autonomic symptoms, and encephalopathy. Flunarizine provided no benefit, while levodopa showed initial efficacy that diminished over time. Table 1 outlines the differential diagnoses for PED [2-3].
Results: WES identified the same SCN4A variant (c.3917G>C, p.G1306A, rs80338792) in both cases. Careful reassessment of the patients’ phenomenology revealed features consistent with myotonia rather than true dystonia. Both cases demonstrated clear exercise-related symptom exacerbation, suggestive of a temperature-sensitive channelopathy affecting Nav1.4 sodium channels.
Conclusion: These cases highlight the potential misclassification of myotonic channelopathies as expressions of dystonia. The G1306A variant in SCN4A likely creates temperature-sensitive alterations in channel permeability, where exercise-induced metabolic changes and increased body temperature modify channel activity. This pathophysiological mechanism explains the exercise-triggered symptoms and has important therapeutic implications, as treatments for channelopathies differ from those for dystonia. Recognizing the myotonic nature of these presentations may guide more effective therapeutic approaches targeting sodium channel dysfunction.
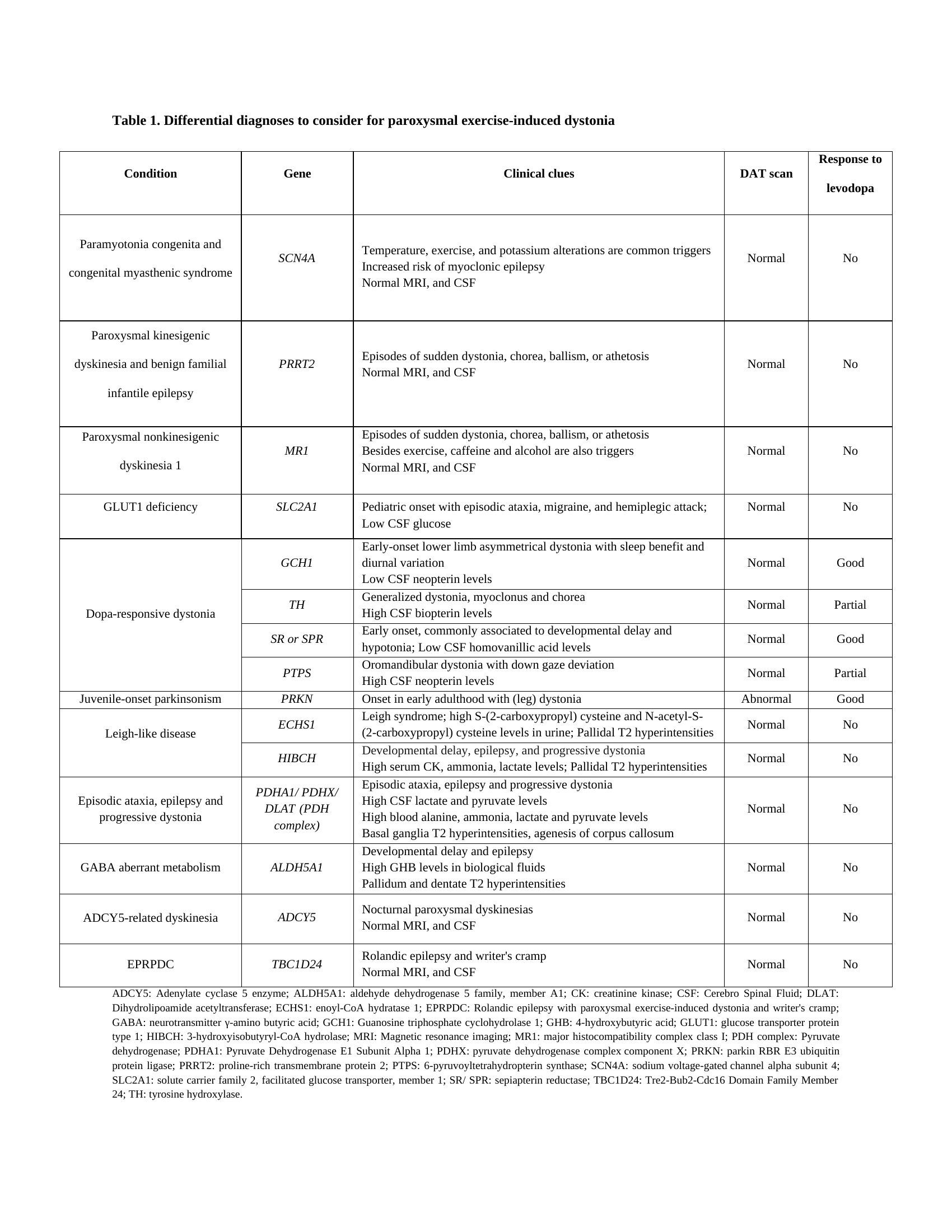
Table 1
References: 1. Sugiura Y, Aoki T, Sugiyama Y, Hida C, Ogata M, Yamamoto T. Temperature-sensitive sodium channelopathy with heat-induced myotonia and cold-induced paralysis. Neurology. 2000 Jun 13;54(11):2179-81. doi: 10.1212/wnl.54.11.2179.
2. Salles PA, Terán-Jimenez M, Vidal-Santoro A, Chaná-Cuevas P, Kauffman M, Espay AJ. Recognizing Atypical Dopa-Responsive Dystonia and Its Mimics. Neurol Clin Pract. 2021 Dec;11(6):e876-e884. doi: 10.1212/CPJ.0000000000001125.
3. Danti FR, Invernizzi F, Moroni I, Garavaglia B, Nardocci N, Zorzi G. Pediatric Paroxysmal Exercise-Induced Neurological Symptoms: Clinical Spectrum and Diagnostic Algorithm. Front Neurol. 2021 Jun 1;12:658178. doi: 10.3389/fneur.2021.658178.
To cite this abstract in AMA style:
B. Talavera Esperanza, N. Chinchihualpa-Paredes, Z. Yu, A. Herrera, P. Vega, E. Hill, M. Kauffman, A. Espay, L. Marsili. Two Cases of SCN4A Temperature-Sensitive Sodium Channelopathy: From Dystonia to Myotonia [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/two-cases-of-scn4a-temperature-sensitive-sodium-channelopathy-from-dystonia-to-myotonia/. Accessed April 10, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/two-cases-of-scn4a-temperature-sensitive-sodium-channelopathy-from-dystonia-to-myotonia/