Category: Parkinsonism (Other)
Objective: To present a case of atypical parkinsonism likely secondary to normal pressure hydrocephalus (NPH) and a colloid cyst at the foramen of Monro.
Background: NPH is traditionally defined by a triad of gait dysfunction, cognitive decline, and urinary incontinence [1]; however, some authors suggest that parkinsonism may also be part of NPH spectrum [2]. Differentiating between primary parkinsonism and NPH-related motor dysfunction is important, as treatment and prognosis differ significantly.
Method: Case report
Results: A 62-year-old right-handed man presented to an outpatient clinic for the evaluation of slowness of thought, difficulty walking, and recurrent falls, leading to wheelchair dependency. His symptoms began five years before presentation with progressive balance impairment and a tendency to fall backward. Over time, he developed bradykinesia, stiffness in his back in the morning, intermittent moaning during sleep, and occasional falls out of bed.
Examination revealed dysarthria, bradykinesia, axial rigidity, intermittent diplopia, and pooling of saliva in the mouth without frank drooling. Eye movement assessment showed hypometric saccades with limited downgaze, saccadic intrusions, a positive “round-the-house” phenomenon, end-gaze horizontal nystagmus, and mild limitation of downward greater than upward gaze. Montreal Cognitive Assessment yielded a score of 26/30. Muscle tone assessment revealed paratonia in both upper and lower extremities, more pronounced on the right side.
Brain MRI (Figure 1) and CT (Figure 2) showed findings consistent with NPH and a 0.6 mm colloid cyst at the foramen of Monro. The patient was treated with carbidopa/levodopa 25/100 mg, one tablet four times daily, but experienced no clinical improvement. He will be scheduled for a large-volume lumbar puncture to assess potential responsiveness to CSF drainage as a treatment for NPH.
Conclusion: This case emphasizes the difficulty of distinguishing atypical parkinsonism from secondary causes such as NPH. Despite gait impairment, oculomotor dysfunction, and levodopa unresponsiveness, the presence of NPH on MRI and a normal midbrain-to-pons ratio raise concerns for an alternative or overlapping etiology. Further evaluation via CSF drainage will help clarify the role of NPH in his symptoms and guide management.
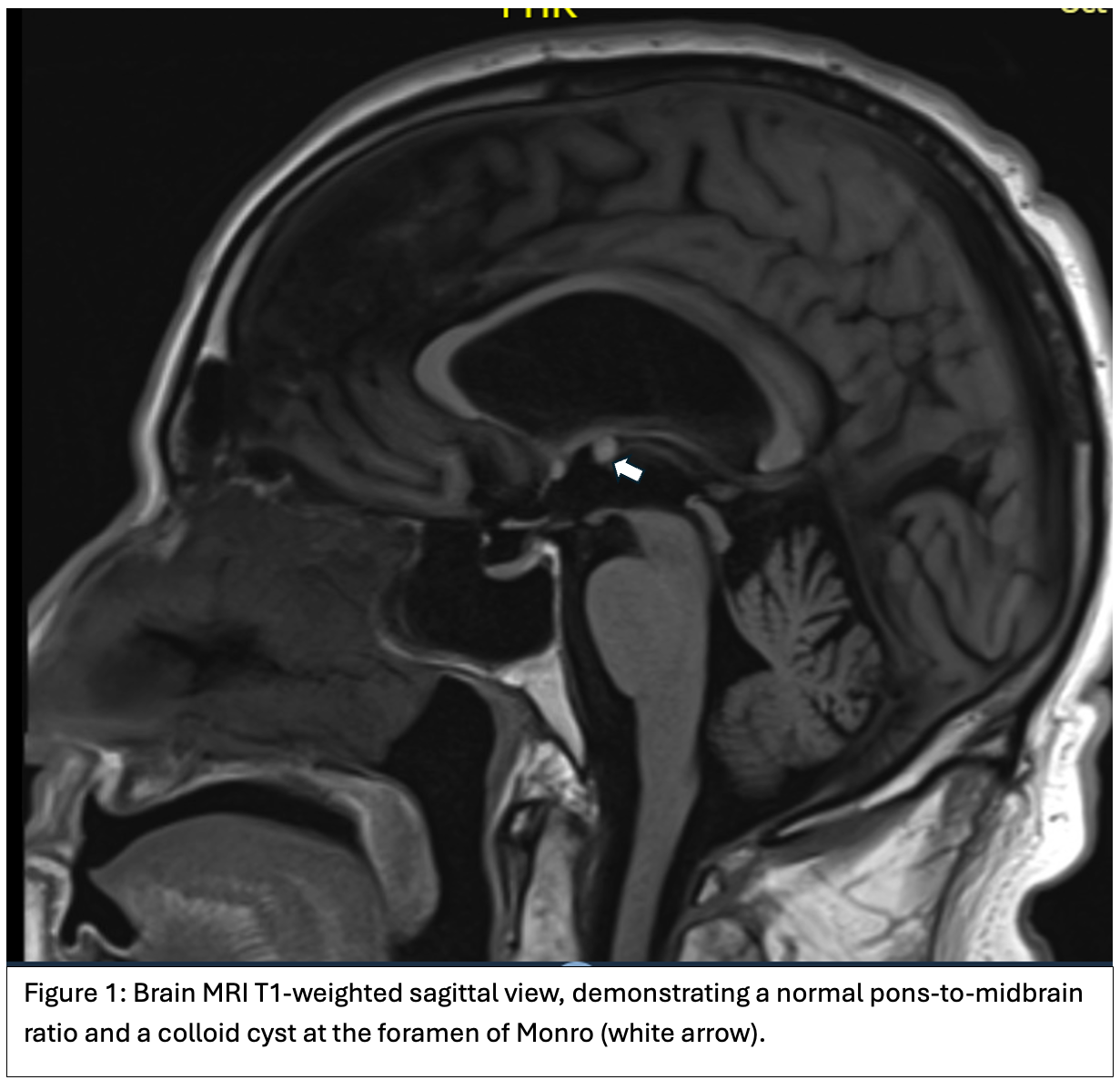
Figure 1
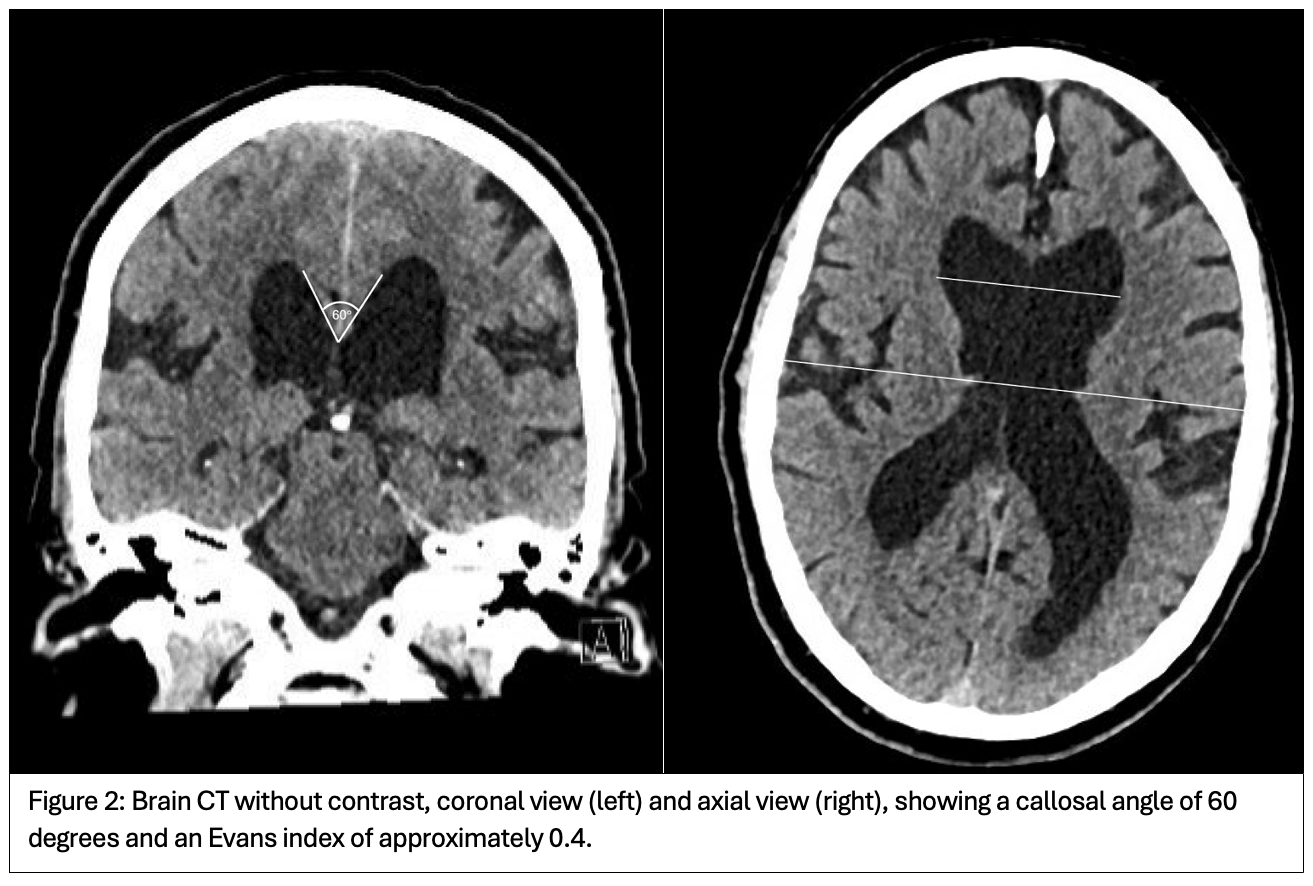
Figure 2
References: 1. Hakim, S., & Adams, R. D. (1965). The special clinical problem of symptomatic hydrocephalus with normal cerebrospinal fluid pressure. Observations on cerebrospinal fluid hydrodynamics. Journal of the neurological sciences, 2(4), 307–327. https://doi.org/10.1016/0022-510x(65)90016-x
2. Mostile, G., Fasano, A., & Zappia, M. (2022). Parkinsonism in idiopathic normal pressure hydrocephalus: is it time for defining a clinical tetrad?. Neurological sciences : official journal of the Italian Neurological Society and of the Italian Society of Clinical Neurophysiology, 43(9), 5201–5205. https://doi.org/10.1007/s10072-022-06119-3
To cite this abstract in AMA style:
QB. Nguyen, O. Los. Atypical Parkinsonism in the Setting of Normal Pressure Hydrocephalus and a Colloid Cyst: Diagnostic Challenge [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/atypical-parkinsonism-in-the-setting-of-normal-pressure-hydrocephalus-and-a-colloid-cyst-diagnostic-challenge/. Accessed July 7, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/atypical-parkinsonism-in-the-setting-of-normal-pressure-hydrocephalus-and-a-colloid-cyst-diagnostic-challenge/