Category: Parkinson's Disease: Surgical Therapy
Objective: To compare motor outcomes, surgical considerations, and follow-up data between unilateral GPi-DBS and GPi-RF pallidotomy in Parkinson’s disease (PD), evaluating their long-term efficacy and safety.
Background: Refinements in neurosurgical techniques have renewed interest in lesioning approaches for PD. With advances in MR-guided focused ultrasound, structures such as the pallidothalamic tract and Forel’s field are reconsidered. Pallidotomy remains an option for cases where DBS is unfeasible, but comparative long-term benefits are unclear. This study assesses whether GPi-RF pallidotomy remains a viable alternative to neuromodulation
Method: A consecutive series of 102 PD patients treated with unilateral GPi-DBS (n=46) or GPi-RF (n=56) between 2017 and 2022 was retrospectively analyzed, ensuring an unbiased selection and real-world outcome comparison. Preoperative and postoperative assessments at 1, 3, and 18 months included motor function (UPDRS-III), activities of daily living (UPDRS-II), dyskinesia (UPDRS-IV), and non-motor symptoms (UPDRS-I)
Results: Demographics: Mean age GPi-DBS: 61.2 ± 6.8 years; GPi-RF: 60.9 ± 7.1 years. Disease duration: ~10 years.
Motor Outcomes: UPDRS-III improvement in both groups, with DBS showing sustained benefit at 18 months (p=0.03). GPi-RF provided faster dyskinesia relief (UPDRS-IV), but long-term differences were minor.
Complications: Minimal surgical complications. Transient effects (6.9%) included dysarthria, headache, and cognitive complaints in DBS; facial paresis and urinary incontinence in RF, resolving within a month. Persistent complications at 6 months: 5.6% in DBS (dysarthria, hardware issues), 2.1% in RF (residual facial paresis).
Safety: A single intracerebral hematoma (<10 mL, 0.9%) in the RF group had no functional consequences.
Conclusion: Both GPi-DBS and GPi-RF are effective and safe. DBS provides sustained benefits, while RF offers faster dyskinesia relief without hardware dependence. Cognitive stability and long-term safety reinforce the continued relevance of lesion-based interventions as a viable alternative for selected PD patients.
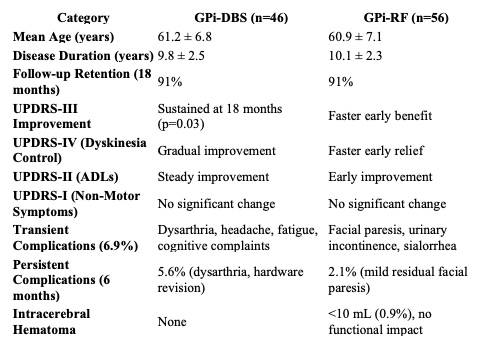
Motor Outcomes GPi-DBS vs. GPi-RF
References: Au KLK, Wong JK, Tsuboi T, et al. Globus Pallidus Internus (GPi) Deep Brain Stimulation for Parkinson’s Disease: Expert Review and Commentary. Neurol Ther. 2021 doi: 10.1007/s40120-020-00220-5.
Strutt AM, Lai EC, Jankovic J, et al. Five-year follow-up of unilateral posteroventral pallidotomy in Parkinson’s disease. Surg Neurol. 2009 . doi: 10.1016/j.surneu.2008.03.039.
Holland MT, Jiao J, Mantovani A, et al. Identifying the therapeutic zone in globus pallidus deep brain stimulation for Parkinson’s disease. J Neurosurg. 2022 doi: 10.3171/2022.5.JNS22152.
Hariz M. Pallidotomy: A “Phoenix the Bird” of Surgery for Parkinson’s Disease? Mov Disord Clin Pract. 2022 . doi: 10.1002/mdc3.13410.
Krishna V, Fishman PS, Eisenberg HM, et al. Trial of Globus Pallidus Focused Ultrasound Ablation in Parkinson’s Disease. N Engl J Med. 2023. doi: 10.1056/NEJMoa2202721.
To cite this abstract in AMA style:
P. Brainer, J. Brainer, A. Brainer, M. Magela, M. Cavalcanti, A. Oliveira, P. Brainer. Pallidotomy Reborn? Revisiting GPi Lesions in the Era of Neuro modulation for Parkinson’s Disease [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/pallidotomy-reborn-revisiting-gpi-lesions-in-the-era-of-neuro-modulation-for-parkinsons-disease/. Accessed July 10, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/pallidotomy-reborn-revisiting-gpi-lesions-in-the-era-of-neuro-modulation-for-parkinsons-disease/