Category: Parkinson's Disease: Surgical Therapy
Objective: This study aims to evaluate the role of intraoperative neurophysiological monitoring, specifically microelectrode recording (MER) and test stimulation, in optimizing electrode placement for deep brain stimulation (DBS) in Parkinson’s disease (PD).
Background: DBS of the Subthalamic Nucleus (STN) is an established treatment for advanced PD. Its success largely depends on precise electrode placement. Two targeting strategies exist: imaging-based (MRI/CT-guided) and neurophysiological (MER-guided). MER identifies STN borders through characteristic firing patterns, allows real-time adjustments, and helps avoid stimulation-related side effects. However, its necessity is debated due to advancements in imaging, increased surgical time, and potential variability.
Method: We conducted a longitudinal analysis on three female PD patients undergoing STN-DBS at “Arcispedale S. Anna,” Ferrara (2024). Preoperative evaluations covered clinical, cognitive, psychiatric, non-motor, and quality-of-life assessments (UPDRS-III, MoCA, NPI, NMSS, PDQ-39, LEDD). Surgery used MRI-CT fusion imaging for initial targeting, followed by MER (three trajectories) to map STN activity and intraoperative test stimulation to assess clinical benefit and side effects. Final electrode placement was guided by MER findings, confirmed via postoperative imaging.At 1 month, postoperative imaging reconstruction was done for all three patients, and a comparison between MER-guided electrode placement and the real placement obtained by reconstruction confirmed the accuracy of MER-guided implantation.
Results: The integration of intraoperative microelectrode recording (MER) with postoperative imaging reconstructions revealed a high concordance between neurophysiological mapping and final electrode placement. This alignment was associated with superior clinical outcomes, confirming the predictive value of MER in optimizing STN-DBS targeting.
At three months post-activation, all patients demonstrated substantial improvements in motor function, with marked reductions in UPDRS-III scores and a dramatic decrease in motor fluctuations and dyskinesias. LEDD decreased significantly and non-motor symptoms and quality of life improved dramatically.
Conclusion: Intraoperative neurophysiology via MER enhances targeting precision in STN-DBS, leading to improved motor, non-motor, and quality-of-life outcomes in PD patients.
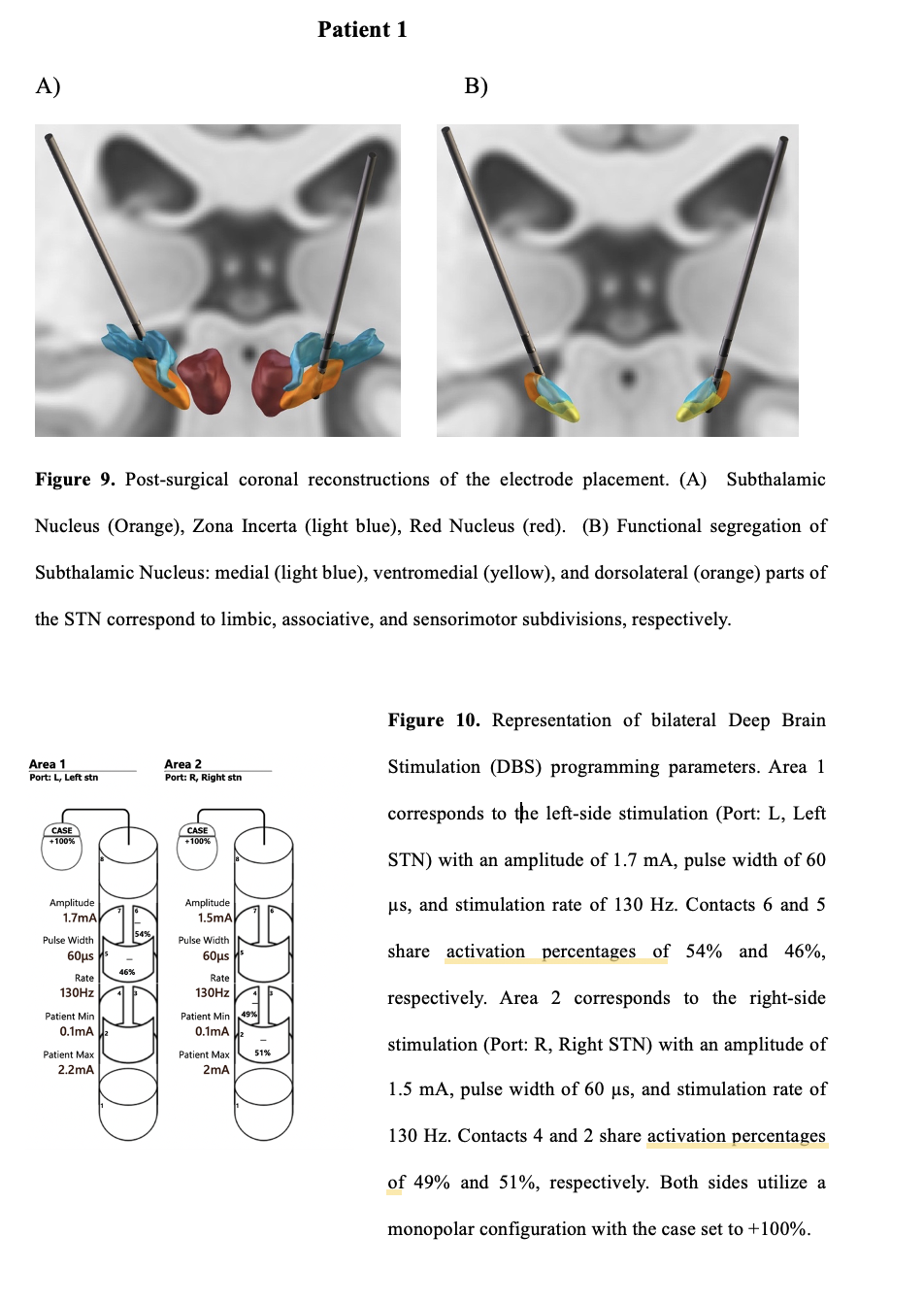
Patient 1 reconstruction and DBS programming
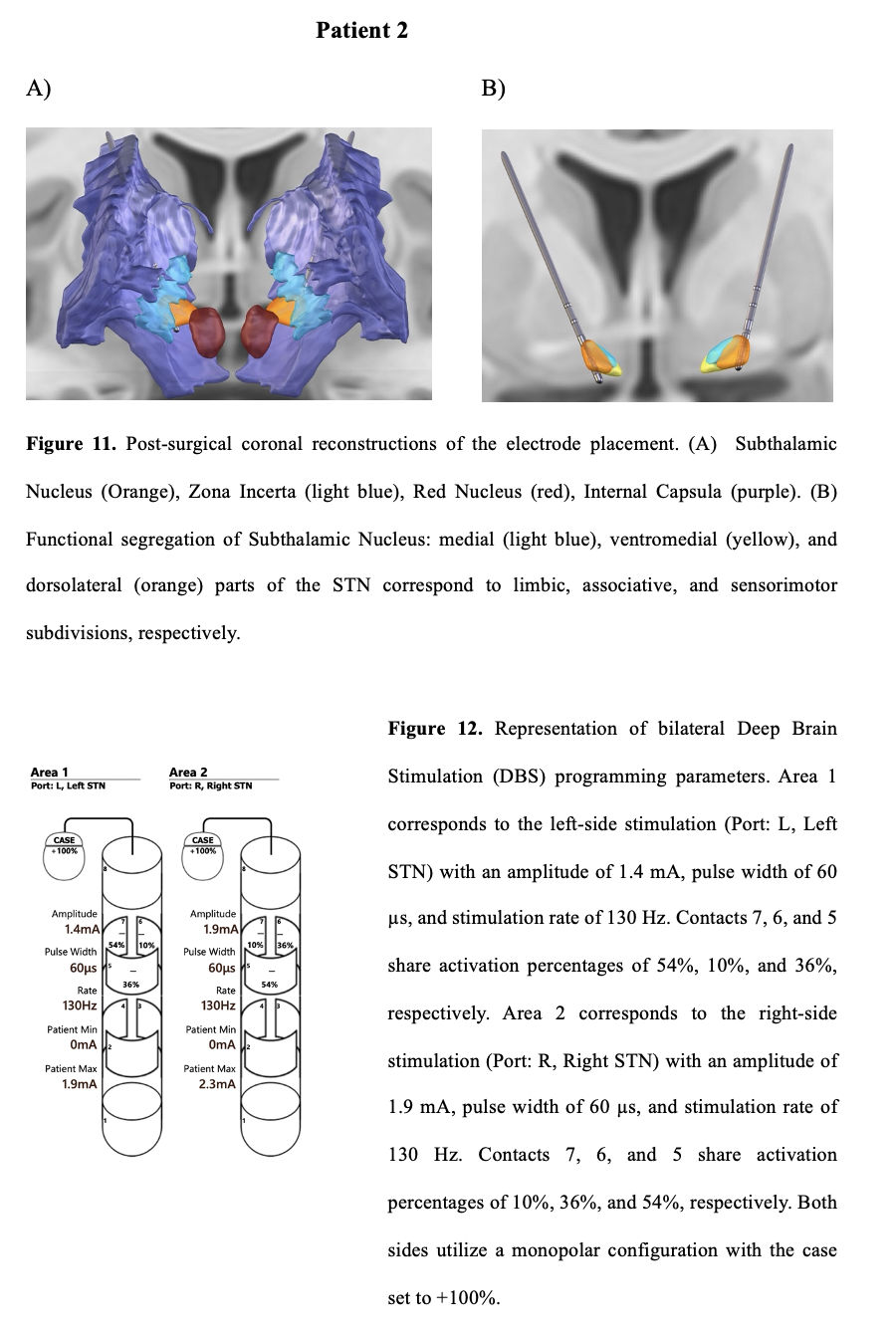
Patient 2 reconstruction and DBS programming
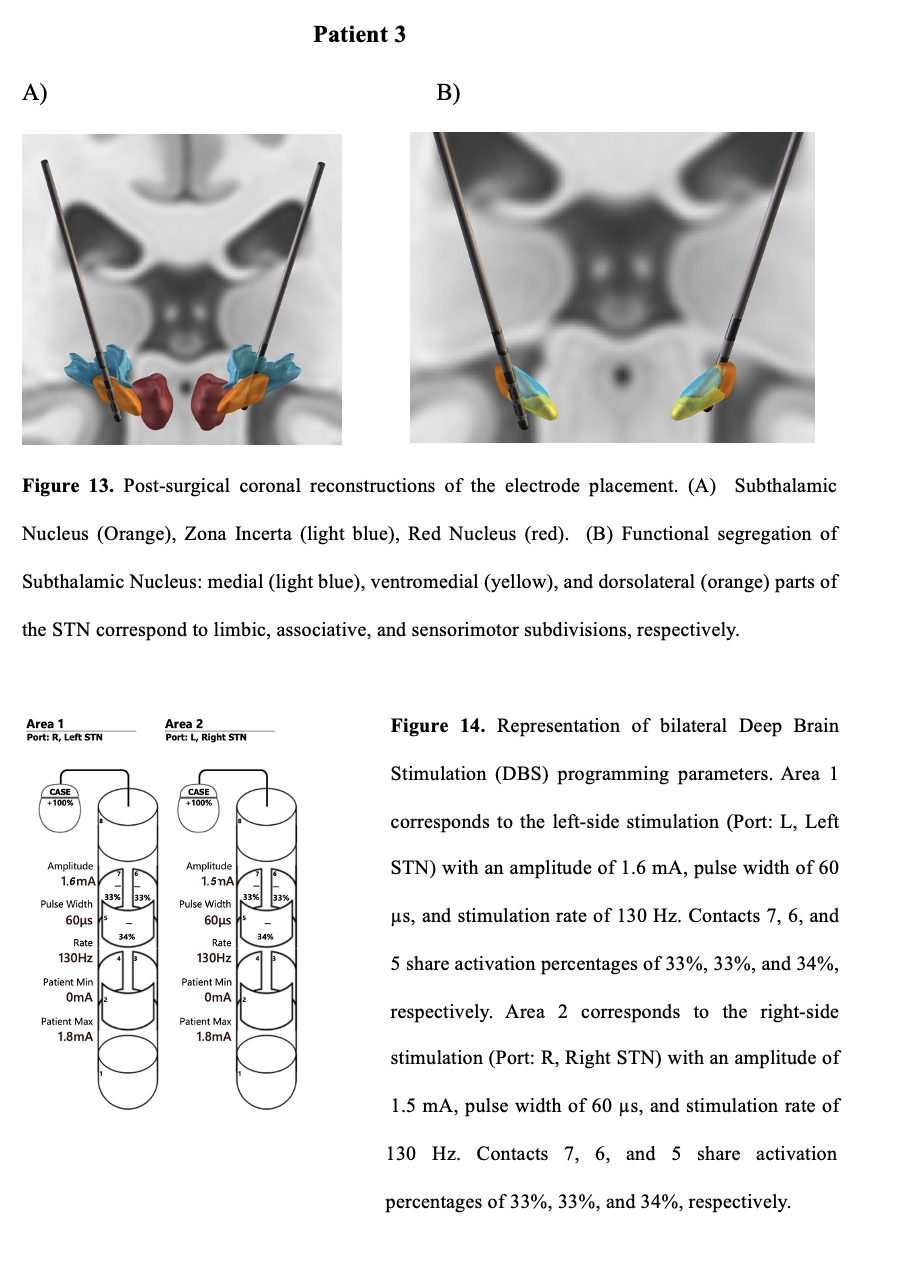
Patient 3 reconstruction and DBS programming
To cite this abstract in AMA style:
M. de Rosa, A. Gozzi, S. Sensi, M. Sensi. Optimizing Electrode Placement in STN-DBS for Parkinson’s Disease: The Added Value of Intraoperative Neurophysiological Monitoring [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/optimizing-electrode-placement-in-stn-dbs-for-parkinsons-disease-the-added-value-of-intraoperative-neurophysiological-monitoring/. Accessed July 10, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/optimizing-electrode-placement-in-stn-dbs-for-parkinsons-disease-the-added-value-of-intraoperative-neurophysiological-monitoring/