Objective: We present a challenging case of genetic PD who presented with progressive weight loss and constipation despite post-DBS and was found to have malignancy.
Background: Weight changes in Parkinson’s disease (PD) are a complex issue. They occur before the onset of the motor symptoms, with weight loss being prominent. Post-deep brain stimulation (DBS) to the bilateral subthalamic nucleus (STN) or globus pallidum (GPi) for PD has generally reported weight gain. PARK2 mutations – missense, frameshift and truncation mutations have been associated with breast, lung, colorectal, and ovarian cancers though combination with PD is rare
Method: Case report
Results: A 42-year-old male presented with insidious onset asymmetric parkinsonian symptoms for 10 years (left more than right) with posturing of left arm and leg at night. Clinical evaluation showed a levodopa responsive young-onset dystonia-parkinsonism (UPDRS III motor OFF score – 57; ON score – 13). Whole exome sequencing showed a disease-causing homozygous contiguous deletion in exon 1 of PARK2(ENST00000366898.1) and exons 1 and 2 of PACRG gene (ENST00000337019.3). He underwent DBS for bilateral STN after 6 years of disease onset. He had progressive constipation with unintentional weight loss even post-DBS and medication modification. He developed acute onset vomiting and abdominal pain. Colonoscopy and abdominal imaging showed polypoidal necrotic anal infiltrative growth with no evidence of metastasis.(Fig1) Biopsy revealed a well-differentiated adenocarcinoma of the rectum. He underwent pre-surgical chemo-radiotherapy with abdominoperineal resection, following which he showed a remarkable weight gain of 10 kgs with a resolution of vomiting and abdominal pain.
Conclusion:
When significant weight loss occurs despite DBS in PD, irrespective of the target, we recommend a comprehensive evaluation for secondary causes like endocrinal abnormalities (hyperthyroidism, diabetes, adrenal insufficiency), infections (tuberculosis and human immunodeficiency virus), psychiatric conditions, gastrointestinal pathologies and malignancies. PARK2 is the most common cause of monogenic PD and can be associated with malignancy.
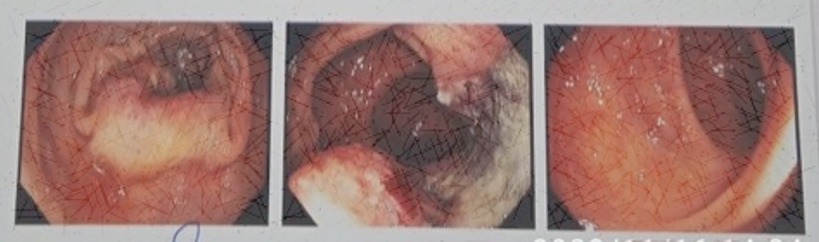
Fig 1- Colonoscopy showing rectal mass
References: Steinhardt J, Lokowandt L, Rasche D, Koch A, Tronnier V, Münte TF, et al. Mechanisms and consequences of weight gain after deep brain stimulation of the subthalamic nucleus in patients with Parkinson’s disease. Sci Rep [Internet]. 2023;13(1):1–11.
Mills KA, Scherzer R, Starr PA, Ostrem JL. Weight change following GPi or STN deep brain stimulation in Parkinson’s disease and dystonia. 2013;90(6):386–93.
Liu X, Le W. Profiling Non-motor Symptoms in Monogenic Parkinson’s Disease. Front Aging Neurosci. 2020;12(October):1–10.
To cite this abstract in AMA style:
R. Kandadai, M. Karri, S. Kola, R. Borgohain, R. Alugolu, P. Vvsrk. Weight loss post deep brain stimulation to bilateral subthalamic nuclei in a Parkinson’s disease with PARKIN mutation – A Harbinger sign of malignancy [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/weight-loss-post-deep-brain-stimulation-to-bilateral-subthalamic-nuclei-in-a-parkinsons-disease-with-parkin-mutation-a-harbinger-sign-of-malignancy/. Accessed July 7, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/weight-loss-post-deep-brain-stimulation-to-bilateral-subthalamic-nuclei-in-a-parkinsons-disease-with-parkin-mutation-a-harbinger-sign-of-malignancy/