Objective: We compared the progression of motor (M) and nonmotor (NM) symptoms in subjects with Parkinson’s Disease (PD) with pre-existing head trauma (HT), with or without loss of consciousness (LoC+/LoC-), to those without pre-exisiting HT from the Parkinson’s Progression Markers Initiative (PPMI) online cohort.
Background: History of HT increases risks of developing PD [1-3]. Prior studies found high odds ratio (OR) between HT, LoC, and PD [2,3]. In the Fox Insight online cohort, severe HT (i.e. with fracture, seizure, or LoC), was associated with faster progression of gait and cognitive impairments [4]. We hypothize that prior HT will be associated with faster progression of M and NM symptoms and even more so for HT with a LoC.
Method: We used the self-reported Head Trauma Questionnaire to separate PD participants as follows: (HT-/LoC-), (HT+/LoC-), (HT+/LoC+). Participant with HT only after PD diagnosis were excluded. Baseline to 33 months scores from the MDS-UPDRS Part I, II, and the Geriatric Depression Scale (GDS) were used for M and NM assessments outcomes. We examined their association with linear mixed effects models with HT, LoC, number of lifetime HTs, study visit time (month), time between first HT (years) and PD diagnosis. Motor symptom outcomes were adjusted for sex, baseline age, and medication status. ORs for the likelihood of developing PD based on presence of HT and LOC were calculated.
Results: Participant demographics are shown in Table 1. While the ratio of men:women who denied HT was near equal; women were more than 2x as likely to endorse HT+ LoC+. Our model had the highest explanatory power for MDS-UPDRS Part II score (Table 2.1–2.3). OR was significant for the LoC+ group (OR=1.14, CI=1.06, 1.23) (Table 3). Assessment mean scores with standard errors elucidate variable levels of severity across cohorts (Graph 1.1–1.3).
Conclusion: Pre-existing HT and HT with LoC were associated with worse scores on MDS Parts I and II. There were no differences in speed of progression of PD M and NM symptoms across cohorts. Outcomes remained parallel with the HT+/LoC+ showing worse overall outcomes throughout the whole observation period. Future studies to investigate potential sex-based differences in the prevalence of pre-existing HT and the impact of HT on severity of PD symptoms is warranted.
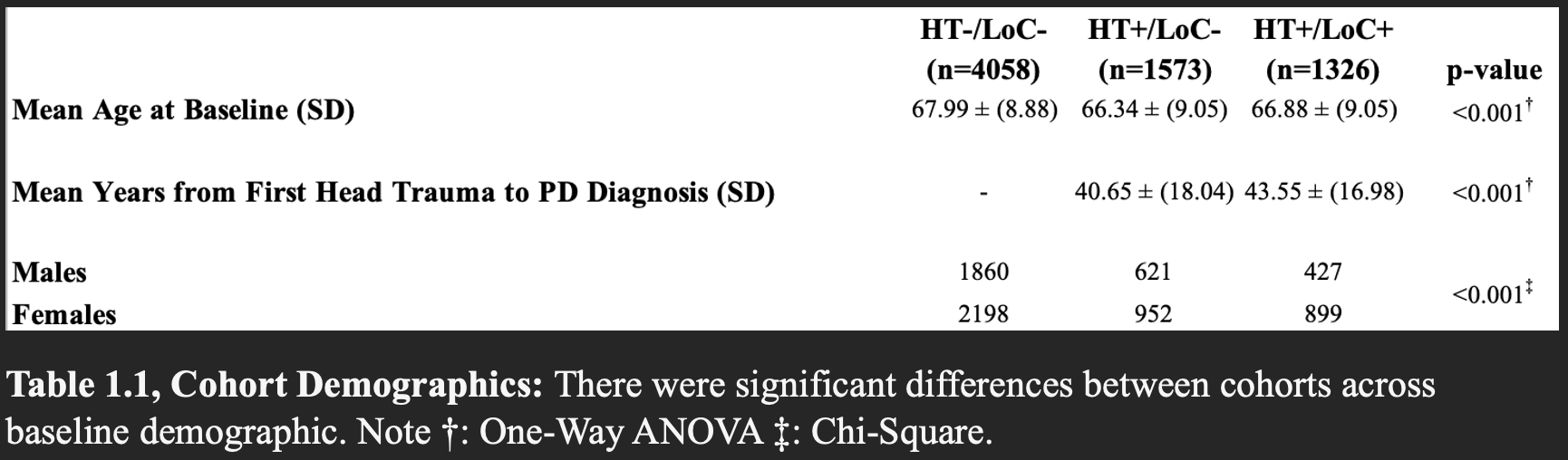
Table 1.1, Cohort Demographics
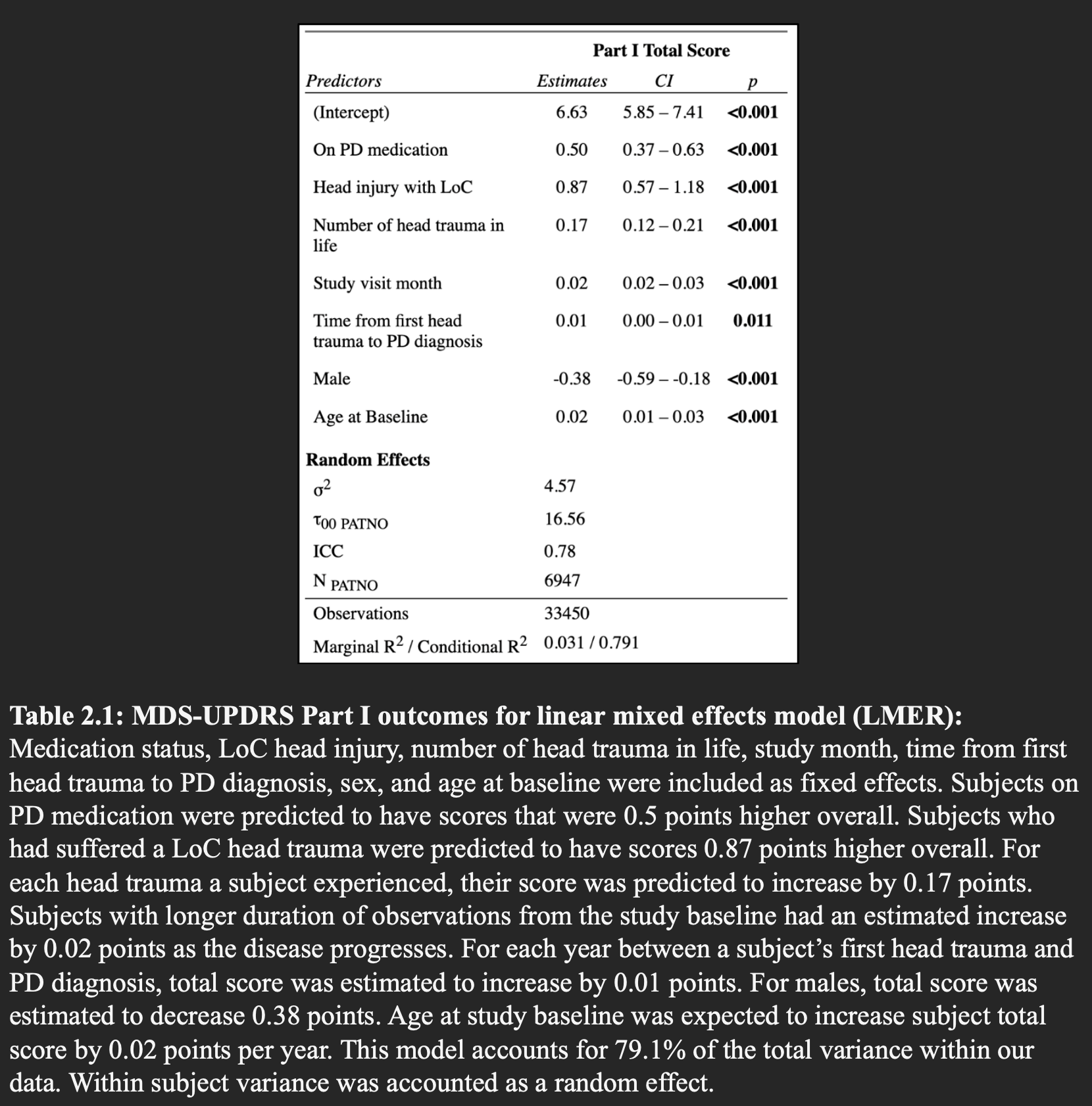
Table 2.1: MDS-UPDRS Part I outcomes
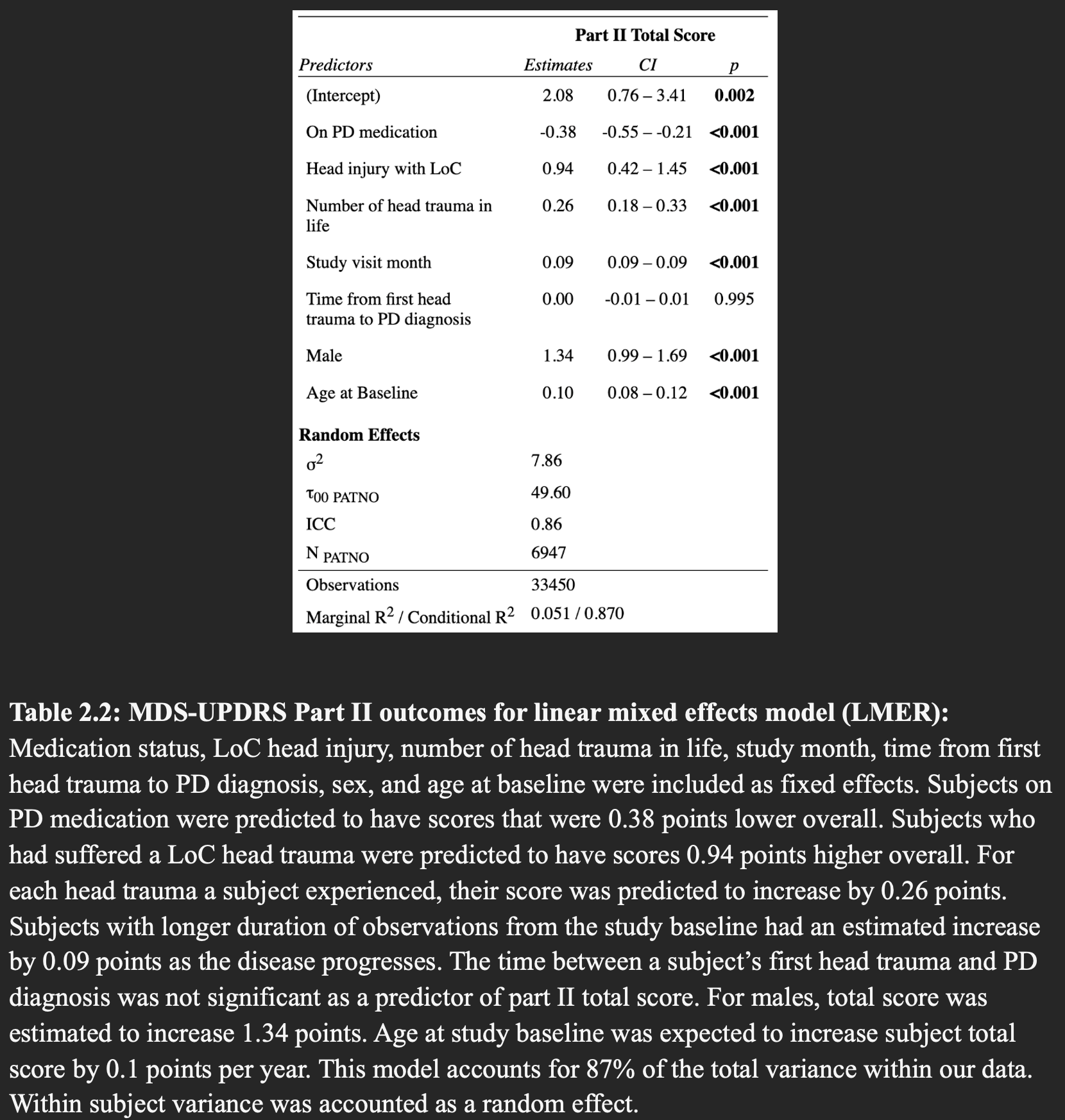
Table 2.2: MDS-UPDRS Part II outcomes
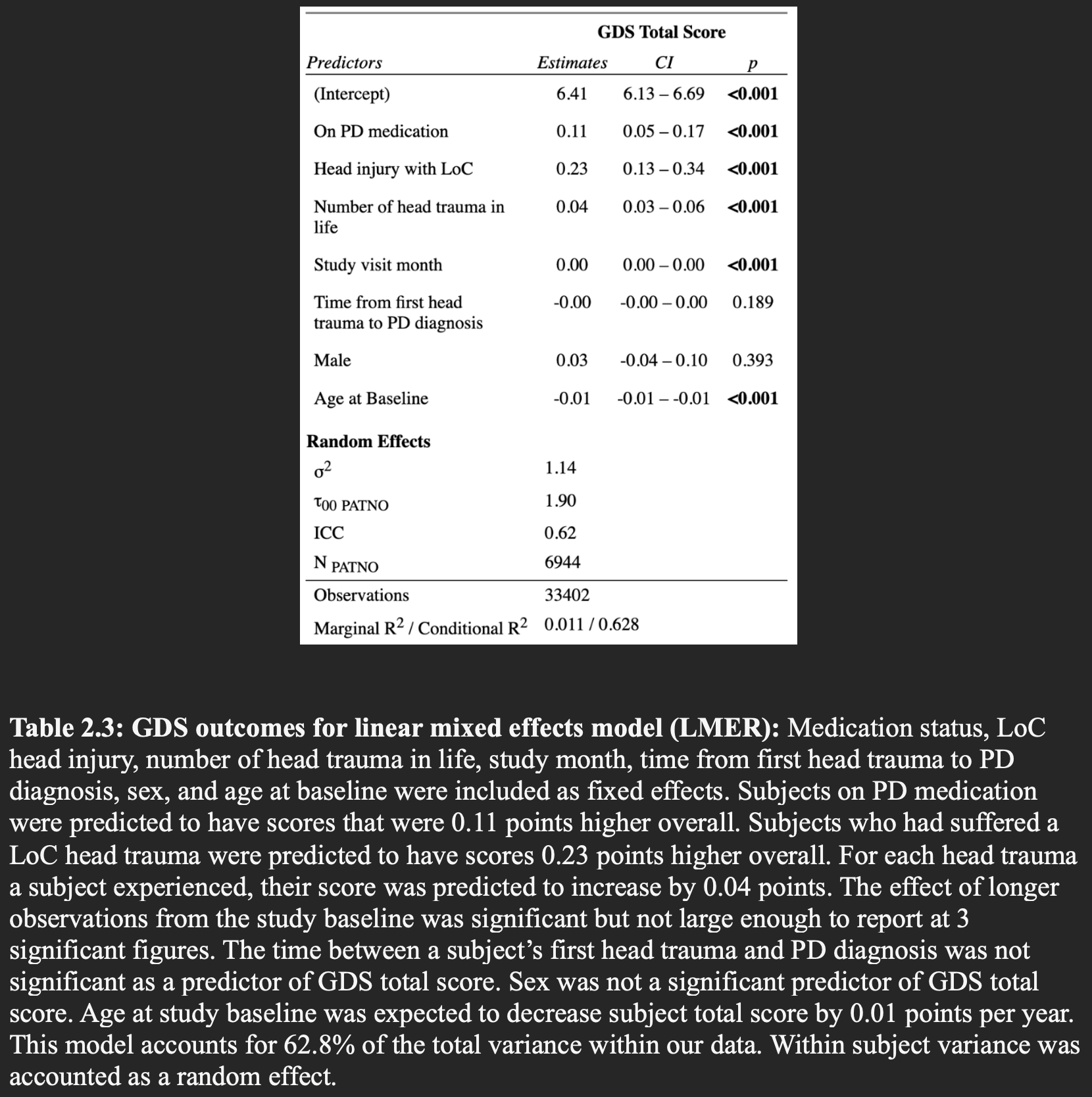
Table 2.3: GDS outcomes
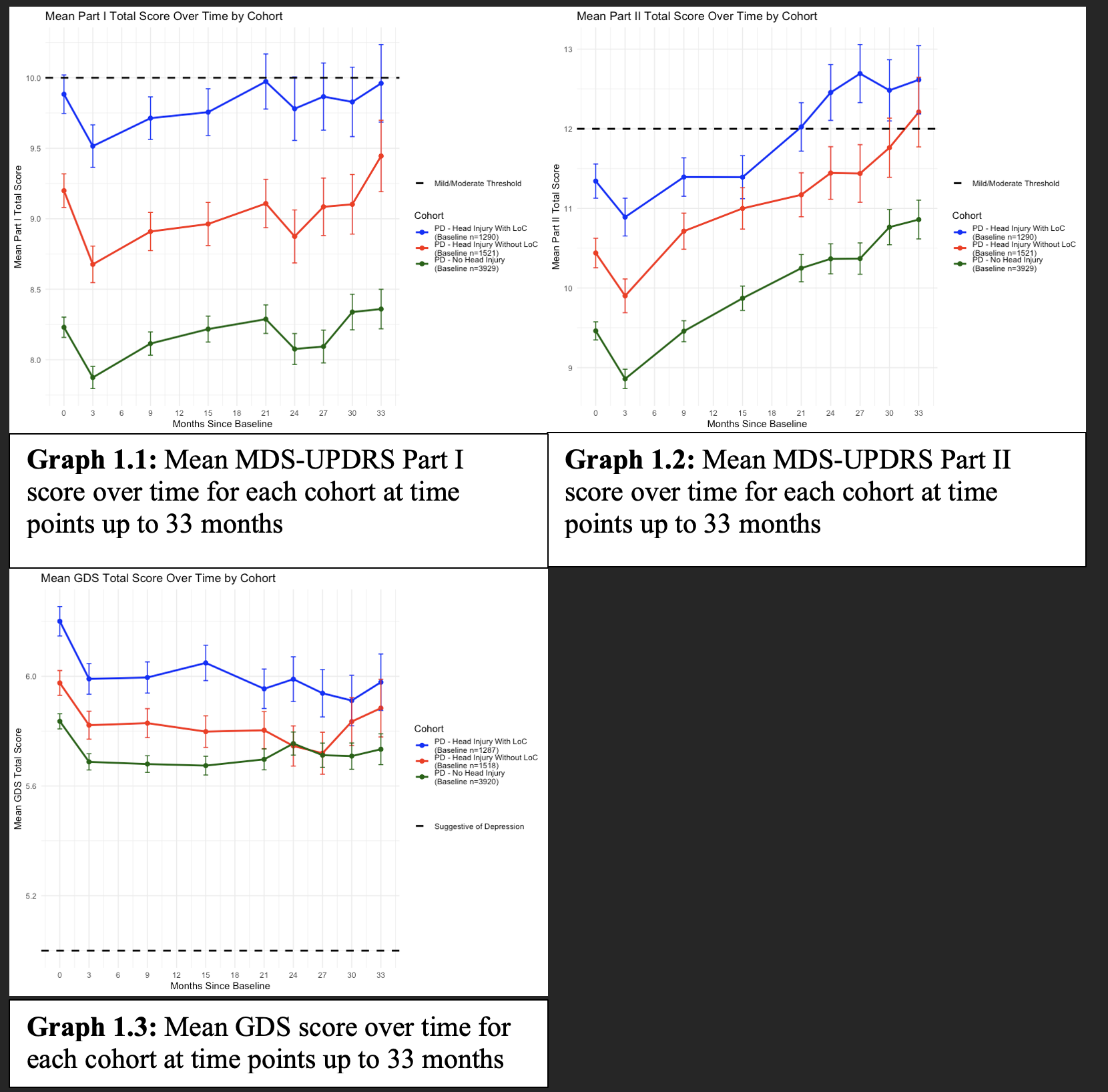
Graph 1.1, Graph 1.2, Graph 1.3
References: 1. Brett BL, Gardner RC, Godbout J, Dams-O’Connor K, Keene CD. Traumatic Brain Injury and Risk of Neurodegenerative Disorder. Biol Psychiatry. 2022;91(5):498-507. doi:10.1016/j.biopsych.2021.05.025
2. Harris MA, Shen H, Marion SA, Tsui JKC, Teschke K. Head injuries and Parkinson’s disease in a case-control study. Occup Environ Med. 2013;70(12):839-844. doi:10.1136/oemed-2013-101444
3. Jafari S, Etminan M, Aminzadeh F, Samii A. Head injury and risk of Parkinson disease: A systematic review and meta-analysis. Movement Disorders. 2013;28(9):1222-1229. doi:10.1002/mds.25458
4. E. Brown, M. San Luciano, S. Goldman, M. Korell, B. Contreras, C. Tanner. Head injury prior to Parkinson’s disease predicts faster self-reported motor and cognitive decline [abstract]. Mov Disord. 2022; 37 (suppl 2). https://www.mdsabstracts.org/abstract/head-injury-prior-to-parkinsons-disease-predicts-faster-self-reported-motor-and-cognitive-decline/. Accessed March 2, 2025.
To cite this abstract in AMA style:
C. Kastoun, R. Rajmohan, J. Ruiz Tejeda, N. Phielipp. Progression of Motor & Non-motor symptoms of Parkinson’s Disease with Prior History of Head Trauma [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/progression-of-motor-non-motor-symptoms-of-parkinsons-disease-with-prior-history-of-head-trauma/. Accessed July 9, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/progression-of-motor-non-motor-symptoms-of-parkinsons-disease-with-prior-history-of-head-trauma/