Category: Choreas (Non-Huntington's Disease)
Objective: To highlight the importance of genetic testing when the clinical symptoms of Chorea Acanthocytosis (ChAc) are misdiagnosed as functional movement disorder (FMD).
Background: ChAc is a rare progressive neurodegenerative condition presenting with movement abnormalities. Patients often manifest psychiatric disturbances, seizures and self-mutilative behaviors. Peripheral blood smear shows acanthocytes and caudate degeneration may present on neuroimaging. Patients often present with variable symptoms which can mimic FMD. Differential diagnoses of ChAC encompass McLeod syndrome, pantothenate kinase-associated neurodegeneration, Huntington’s disease-like 2, Wilson disease, and drug-induced or infectious conditions. Early genetic testing is crucial for effective treatment and long-term prognosis.
Method: Case Report
Results: 29-year-old right-handed Hispanic man presented with abnormal movements and recent onset of seizures. Patients’ birth and early development was normal. During early teenage years there were anger, behavioral, and external psychosocial issues requiring psychotropics. At age 21, he developed progressive involuntary movements, declining cognition, and generalized seizures. Worsening psychosis led to several hospitalizations for suicidal and homicidal ideation. Patient was seen by different neurologists, diagnosed with TD vs FMD. The patient was seen for second opinion and physical exam revealed generalized chorea, dystonic posturing, dysarthria, and oral-facial dyskinesias. Laboratory tests were within normal limits, brain MRI showed caudate atrophy, and prolonged EEG captured one focal onset seizure with transient impairment of cerebral function localizing to bilateral frontotemporal regions. While his seizures improved with oxcarbazepine, his chorea remained bothersome despite trial of Risperidone, Olanzapine and Deutetrabenazine. Genetic testing was initiated, yielding VPS13A mutation, confirming autosomal recessive ChAc.
Conclusion: This is a unique case of ChAc initially misdiagnosed as FMD. The diagnostic challenges encountered were due to motor manifestations overshadowed by psychological symptoms. Our case highlights the importance of genetic testing for young patients with chorea and chronic psychiatric symptoms. Early genetic testing facilitates targeted interventions and prognostication alongside genetic counseling.
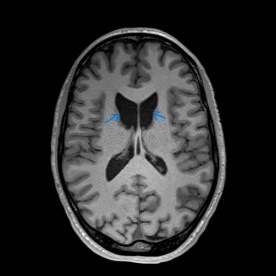
Early Bilateral Caudate Atrophy
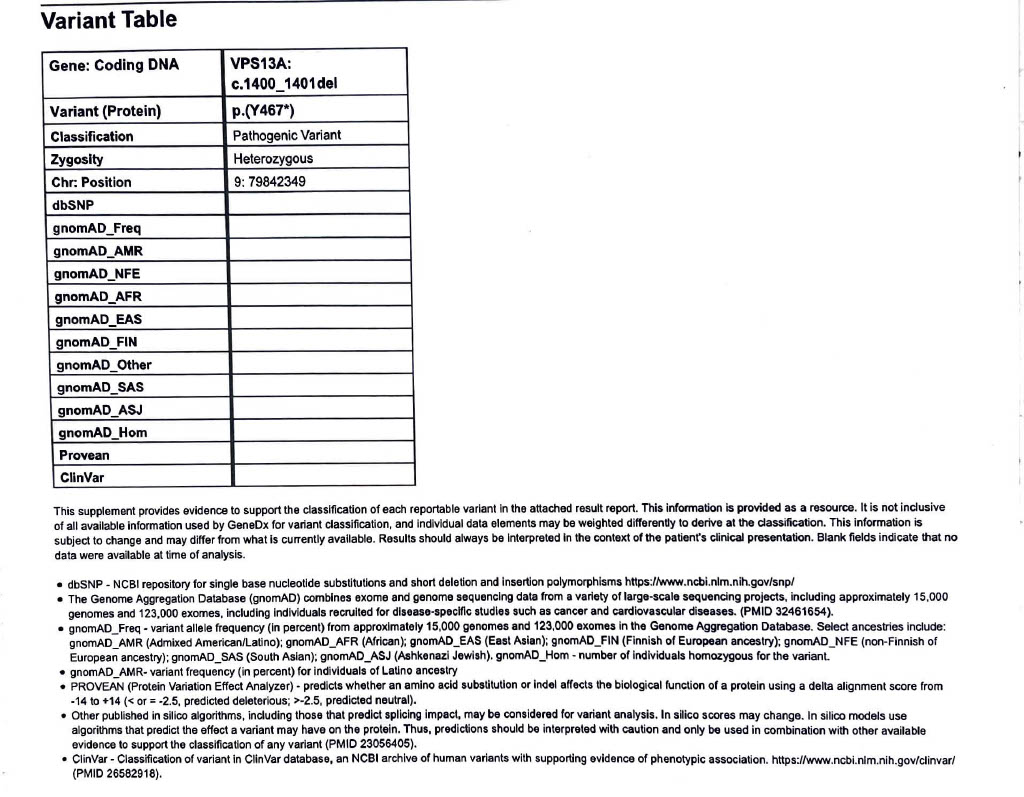
Genetic Testing Report: (+) VPS13A Mutation
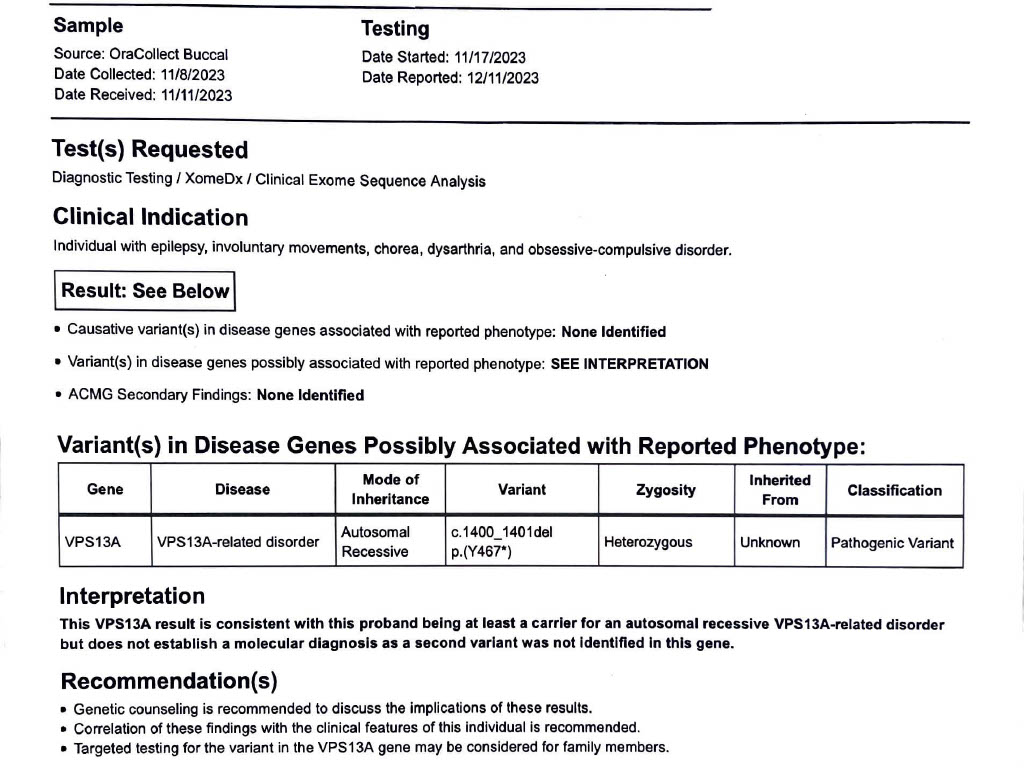
Genetic Testing Report: (+) VPS13A Mutation
References: [1] Peikert K, Danek A, Hermann A. Current state of knowledge in Chorea-Acanthocytosis as core Neuroacanthocytosis syndrome. Eur J Med Genet. 2018 Nov;61(11):699-705. doi: 10.1016/j.ejmg.2017.12.007. Epub 2017 Dec 16. PMID: 29253590.
[2] Jung HH, Danek A, Walker RH. Neuroacanthocytosis syndromes. Orphanet J Rare Dis. 2011 Oct 25;6:68. doi: 10.1186/1750-1172-6-68. PMID: 22027213; PMCID: PMC3212896.
To cite this abstract in AMA style:
A. Crutchfield, N. Reddy, A. Ahmed, M. Lotia. Chorea Acanthocytosis Misdiagnosed as Functional Movement Disorder [abstract]. Mov Disord. 2024; 39 (suppl 1). https://www.mdsabstracts.org/abstract/chorea-acanthocytosis-misdiagnosed-as-functional-movement-disorder/. Accessed August 11, 2026.« Back to 2024 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/chorea-acanthocytosis-misdiagnosed-as-functional-movement-disorder/