Session Information
Date: Wednesday, September 25, 2019
Session Title: Phenomenology and Clinical Assessment of Movement Disorders
Session Time: 1:15pm-2:45pm
Location: Les Muses Terrace, Level 3
Objective: The aim of this study is to present a case series of patients affected by movement disorders and Fahr’s disease or Primary Familial Brain Calcification (PFBC), analysing clinical presentation, radiological features and genetic profiles.
Background: PFBC is a rare neurological disease characterized by idiopathic calcification of basal ganglia [1]. Five genes have been identified to cause the disease, namely SLC20A2, PDGFR, PDGFRB, XPR1 and MYORG [2]. Even if almost all these genes are involved in phosphate-calcium metabolism or in brain blood barrier permeability, the exact pathogenesis of PFBC is still unknown and the treatment is only symptomatic [3].
Method: From our movement disorders database, we selected patients with basal ganglia calcification. Firstly, we analysed the clinical and radiological data; secondly, we performed a genetic panel for 96 genes associated with Parkinson’s disease, Fahr’s disease, lysosomal and mitochondrial diseases, dystonia, dementia and neurodegeneration with brain iron accumulation (NBIA).
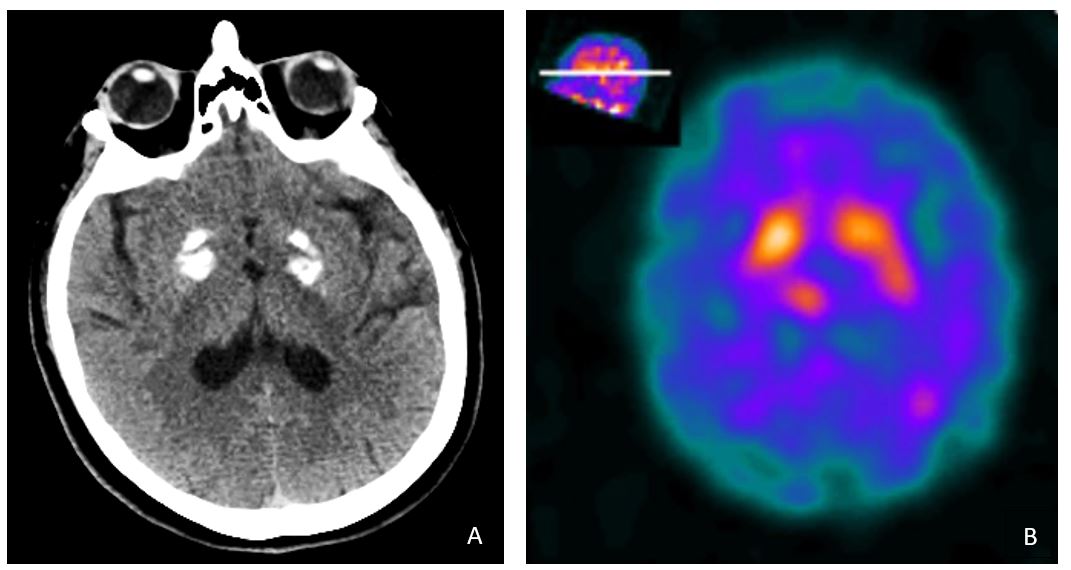
Results: The case series from our database showed ten patients, five males and five females. The mean (±SD) age at onset of symptoms was 63 (± 8.8) years. Clinically, the most frequent neurological symptoms were rigidity (60%), postural instability (60%) and tremor (50%), while depression and anxiety figured as the main psychiatric disorders; furthermore, two-thirds of patients receiving levodopa showed dyskinesias [figure 1]. The globus pallidus was the main radiological site affected by calcifications (70%), followed by the cerebellum (40%). Five patients had a positive family history for movement disorders, but in only one patient a causative mutation for Fahr’s disease was found. DaT-SPECT was performed in five patients and showed significant bilateral lower striatal DaT uptake; however, in all these cases one side resulted more involved than the contralateral [figure 2].
Conclusion: Although the genetic knowledge of PFBC is increasing, most patients do not show mutations in genes known to cause the disease and exhibit various clinical features, whose neuropathogenesis remains poorly defined. Considering that basal ganglia calcification on CT scans are extremely symmetrical, the finding of lateralization in the DaT-SPECT sequences complicates the understanding of the pathogenetic role of calcifications.

References: [1] Manyam BV, Walters AS, Narla KR. Bilateral striopallidodentate calcinosis: clinical characteristics of patients seen in a registry, (2001). Movement disorders: official journal of the Movement Disorder Society;16(2):258–264. doi: 10.1002/mds.1049. [2] Xiang-Ping Yao, Xuewen Cheng, Chong Wang, Miao Zhao, Xin-Xin Guo, Hui-Zhen Su, Lu-Lu Lai, Xiao-Huan Zou, Xue-Jiao Chen, Yuying Zhao, En-Lin Dong, Ying-Qian Lu, Shuang Wu, Xiaojuan Li, Gaofeng Fan,Hongjie Yu,6Jianfeng Xu, Ning Wang, Zhi-Qi Xiong,2, Wan-Jin Chen, (2018). Biallelic Mutations in MYORG Cause Autosomal Recessive Primary Familial Brain Calcification, Neuron, 98 (6), pp. 1116-1123.e5. [3] Manyam BV, (2005). What is and what is not ‘Fahr’s disease’, Parkinsonism Relat Disord.;11(2):73–80
To cite this abstract in AMA style:
F. Arienti, G. Franco, E. Monfrini, A. Seresini, A. Di Fonzo. Clinical, genetic and radiological characterization of patients with movement disorders and basal ganglia calcification [abstract]. Mov Disord. 2019; 34 (suppl 2). https://www.mdsabstracts.org/abstract/clinical-genetic-and-radiological-characterization-of-patients-with-movement-disorders-and-basal-ganglia-calcification/. Accessed August 8, 2026.« Back to 2019 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/clinical-genetic-and-radiological-characterization-of-patients-with-movement-disorders-and-basal-ganglia-calcification/