Category: Ataxia
Objective: To delineate clinical, radiological and genetic profile of patients with ataxia with oculomotor apraxia type-2 (AOA2) in Indian cohort.
Background: AOA2 is a relatively rare autosomal recessive progressive cerebellar ataxia, caused by mutation/s in SETX gene, encoding senataxin protein. Clinicoradiological and genetic data of AOA2 from Indian population is limited. Therefore, it is important to understand its key clinical and radiological features along with molecular characteristics.
Method: Patients with clinical and radiological features suggestive of AOA2 and confirmed with genetic testing were included from three different centers from India.
Results: Total four patients (male: female= 1:1) with clinico-radiological profile consistent with AOA2 along with pathogenic mutations in SETX gene were included. The clinical, radiological as well as genetic mutation details of all 4 patients are depicted in [Table 1]. All patients had relatively later age at onset (mean age at onset- 22 years) as compared to ataxia telangiectasia (AT) and Ataxia with oculomotor apraxia type-1 (AOA1). All four patients showed classic tetrad of slowly progressive cerebellar ataxia with dysarthria, evidence of cerebellar atrophy on MRI, high serum AFP levels and sensorimotor axonal polyneuropathy on NCS testing. Only two out of four patients showed evidence of oculomotor apraxia on eye movement examination, consistent with global data. Out of 4 patients, only one patient had evidence of dystonia in upper extremities. The genetic profile of patients delineated all mutations to be located within either N-terminal (protein interaction) domain or C-terminal helicase domain in SETX gene. Two patients had pathogenic homozygous deletions, while one patient had a pathogenic homozygous mutation in the gene and another patient had pathogenic compound heterozygous mutations (confirmed in parents).
Conclusion: This case series highlights the key clinical and radiological features of AOA2. It delineates the importance of high clinical suspicion towards AOA2 in any patient presenting with slowly progressive recessive cerebellar ataxia, Serum AFP testing (including absolute value) is the key to differentiate it from other causes of recessive cerebellar ataxia. Presence of superior cerebellar atrophy on brain MRI can be a clue to diagnosis of AOA2.
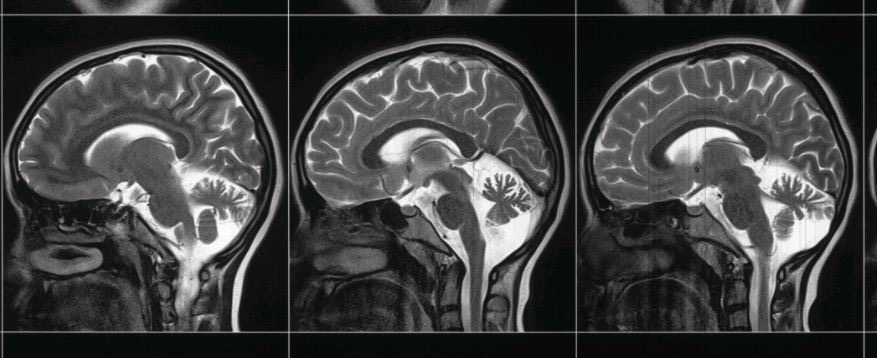
Figure 1
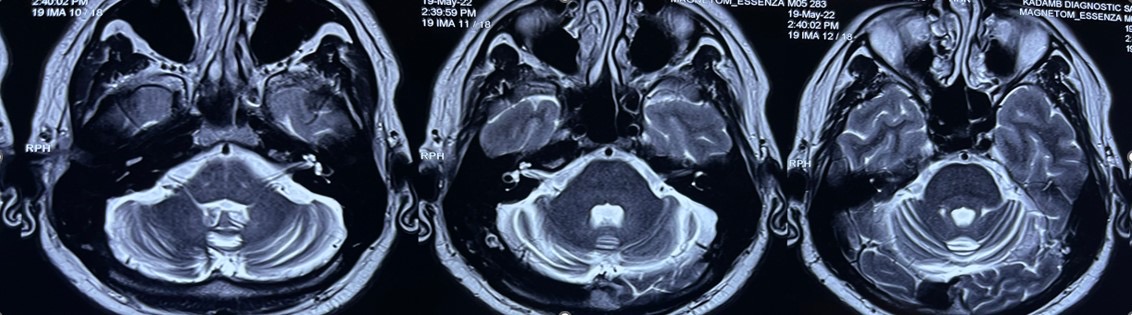
Figure 2
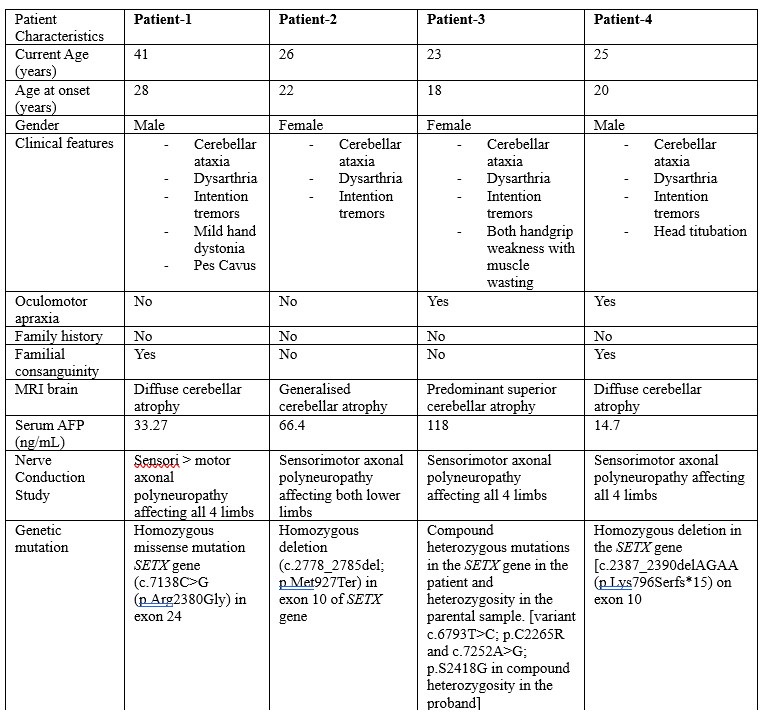
Table 1
References: [1] Renaud M, Tranchant C, Koenig M, Anheim M. Autosomal Recessive Cerebellar Ataxias With Elevated Alpha-Fetoprotein: Uncommon Diseases, Common Biomarker. Mov Disord. 2020 Dec;35(12):2139-2149
[2] Anheim M, Monga B, Fleury M, Charles P, Barbot C, Salih M et al. Ataxia with oculomotor apraxia type 2: clinical, biological and genotype/phenotype correlation study of a cohort of 90 patients. Brain. 2009 Oct;132(Pt 10):2688-98. [3] Brugger F, Schüpbach M, Koenig M, Müri R, Bohlhalter S, Kaelin-Lang A et al. The Clinical Spectrum of Ataxia with Oculomotor Apraxia Type 2. Mov Disord Clin Pract. 2014 May 27;1(2):106-109. [4] Paucar M, Taylor AMR, Hadjivassiliou M, Fogel BL, Svenningsson P. Progressive Ataxia with Elevated Alpha-Fetoprotein: Diagnostic Issues and Review of the Literature. Tremor Other Hyperkinet Mov (N Y). 2019 Oct 10;9.
To cite this abstract in AMA style:
M. Chandarana, B. Tilva, A. Agarwal, D. Garg. Clinico-radiological and genetic profile of patients with Ataxia with Oculomotor apraxia type-2 (AOA2)- A case series from India [abstract]. Mov Disord. 2024; 39 (suppl 1). https://www.mdsabstracts.org/abstract/clinico-radiological-and-genetic-profile-of-patients-with-ataxia-with-oculomotor-apraxia-type-2-aoa2-a-case-series-from-india/. Accessed July 16, 2026.« Back to 2024 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/clinico-radiological-and-genetic-profile-of-patients-with-ataxia-with-oculomotor-apraxia-type-2-aoa2-a-case-series-from-india/