Category: Parkinson's Disease: Surgical Therapy
Objective: To demonstrate the proof-of-concept of a closed-loop deep brain stimulation (DBS) policy designed to reduce slowness in Parkinson’s disease (PD) by increasing stimulation amplitudes during movement.
Background: Subthalamic DBS is an established treatment for alleviating symptoms of PD, including bradykinesia or slowness of movement. Conventional DBS (cDBS) involves constant stimulation amplitudes, which may lead to sub-optimal treatment due to symptom fluctuations. Adaptive DBS (aDBS) represents an emerging paradigm where stimulation levels are modulated based on feedback signals, potentially improving therapeutic outcomes.
Method: We implanted bilateral Medtronic RC+S neurostimulators and electrocorticography arrays in a patient with PD. Recordings were made from the subthalamic nucleus and sensorimotor cortex while forearm speeds were monitored using wrist-worn accelerometers. We developed and validated an aDBS policy that increased stimulation during forearm movement, both in a short, supervised tapping task and over an 18-day period in an unconstrained, naturalistic setting. The study included two control conditions to which the patient was blinded: cDBS and an inverse aDBS policy where stimulation levels were lowered during movement.
Results: We constructed a machine learning pipeline that identified cortical beta (16-32 Hz) and broadband gamma (52-98 Hz) as the most predictive power bands for movement decoding (balanced accuracy: 0.83 ± 0.03). During the tapping task, the aDBS policy significantly improved forearm speed in both hands compared to the inverse control [Figure 1]. For the left hand, the aDBS policy also produced higher tapping speeds than cDBS. Over the 18-day period, the aDBS policy significantly reduced bradykinesia compared to cDBS, as measured by Parkinson’s KinetiGraph (PKG) watches [Figure 2] and self-reports [Figure 3]. There was no difference in tremor severity between the policies. PKG watches noted a slight increase in dyskinesia severity with aDBS, which was not discernible to the patient based on self-reports. Overall, the patient reported a significant preference for the aDBS policy.
Conclusion: Intracranial neural signals enabled the accurate prediction of real-time, naturalistic forearm movement. Using this as a control signal for closed-loop DBS therapy led to significant improvements in motor function compared to conventional DBS in both acute and chronic settings.
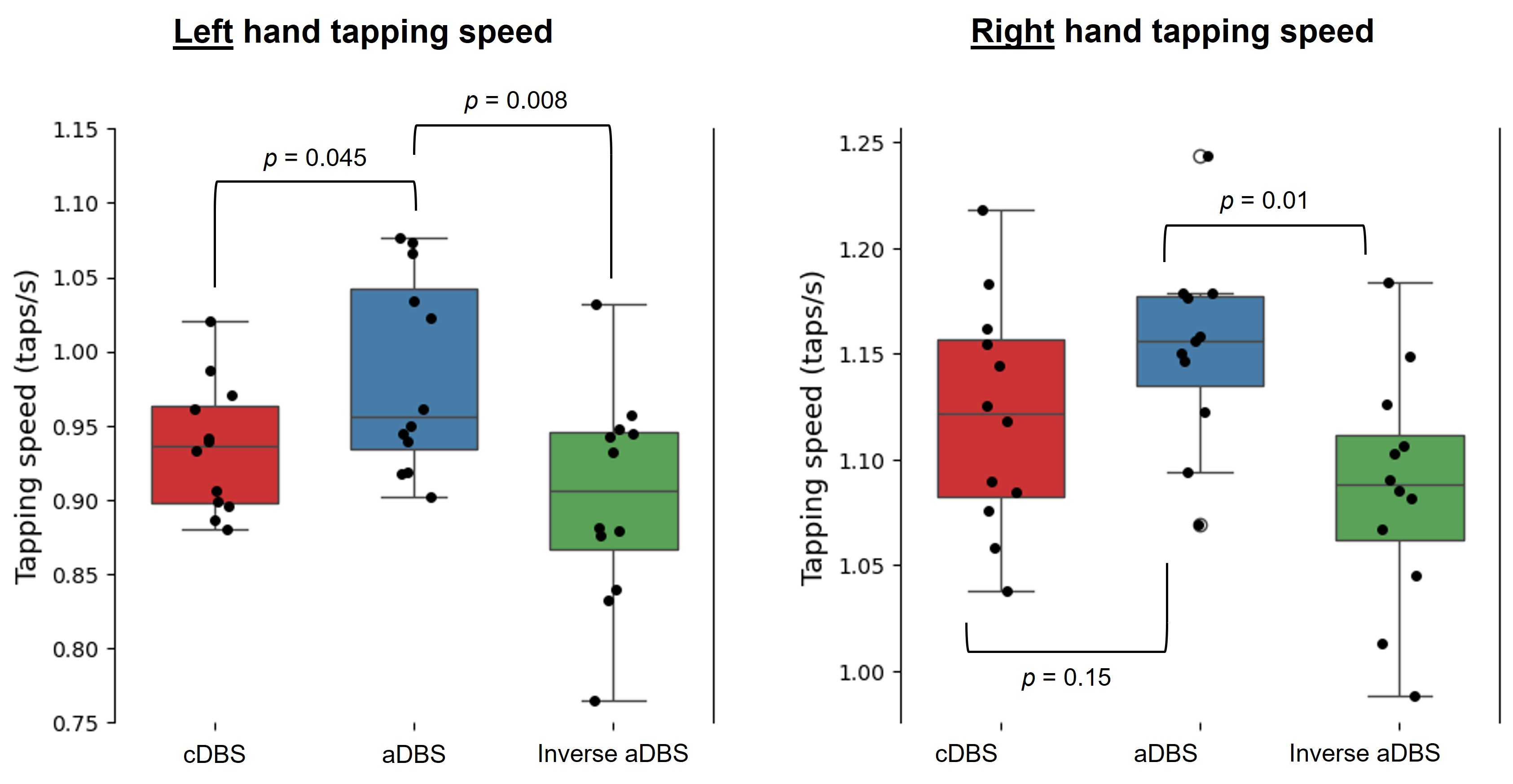
Figure 1: Tapping speeds for left and right hands.
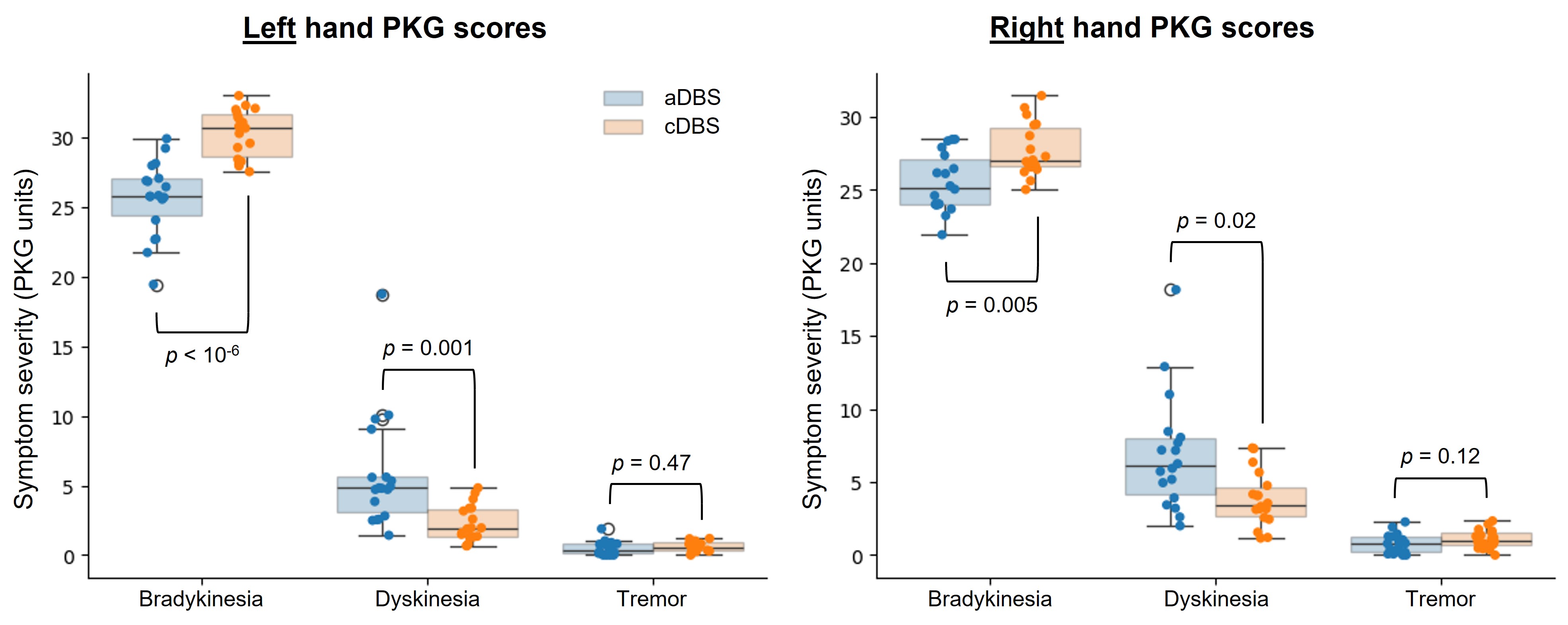
Figure 2: PKG symptom severity scores.
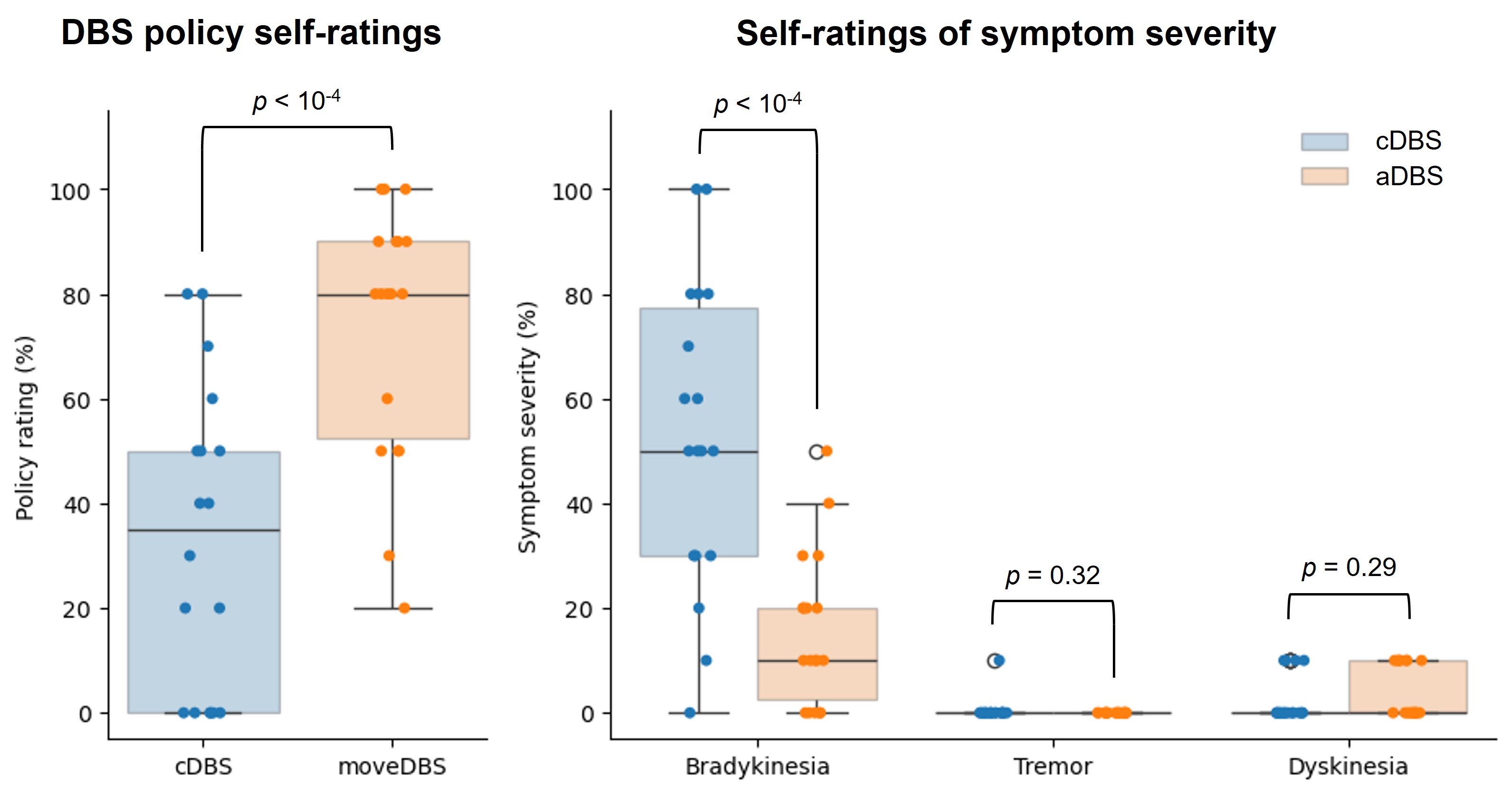
Figure 3: Patient self-ratings.
References: 1. Dixon, T. C. et al. Movement-responsive deep brain stimulation for Parkinson’s Disease using a remotely optimized neural decoder. Preprint at https://doi.org/10.1101/2024.08.14.24312002 (2024).
2. Darbin, O. et al. Subthalamic nucleus deep brain stimulation driven by primary motor cortex γ2 activity in parkinsonian monkeys. Sci Rep 12, (2022).
To cite this abstract in AMA style:
D. Lawrence, P. Starr, S. Little. Decoding Naturalistic Movement for Adaptive Deep Brain Stimulation in Parkinson’s Disease [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/decoding-naturalistic-movement-for-adaptive-deep-brain-stimulation-in-parkinsons-disease/. Accessed April 10, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/decoding-naturalistic-movement-for-adaptive-deep-brain-stimulation-in-parkinsons-disease/