Objective: We report our experience with deep brain stimulation (DBS) using asymmetrical targets in the right and left hemispheres for the treatment of dystonia in a patient with RDP.
Background: Rapid-onset dystonia parkinsonism (RDP/ DYT12) is a rare movement disorder that is caused by mutations in the ATP1A3 gene [3] and is characterized by acute onset of dystonia and parkinsonism which is unresponsive to levodopa. Deep brain stimulation (DBS) of the globus pallidus interna (GPi) or subthalamic nucleus (STN) are both effective in alleviating dystonia however there are no studies stating which of the two is better. A few cases of RDP who underwent DBS have been reported but all of them failed to show significant response to DBS [1][9].
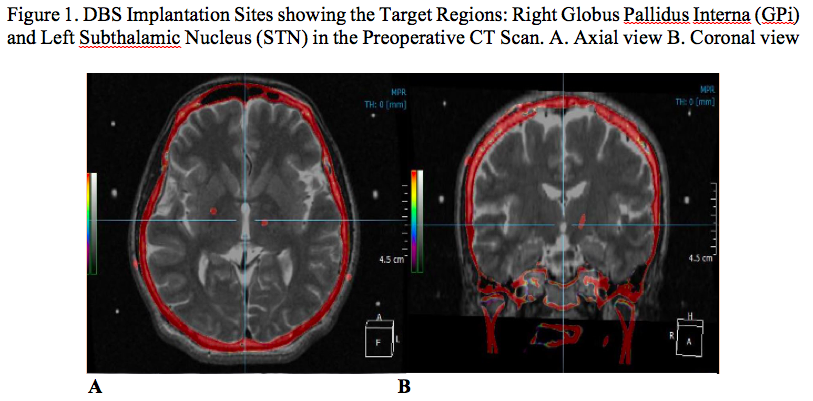
Method: A 49-year-old Korean male with sporadic rapid-onset dystonia parkinsonism (RDP) who initially exhibited sudden onset of dystonia and parkinsonism accompanied by dysarthria and dysphagia. At the age of 39, he underwent deep brain stimulation of the right globus pallidus interna (GPi) and the left subthalamic nucleus (STN) [Figure1]. Modulation of the different stimulation parameters was done to optimize the DBS effect.
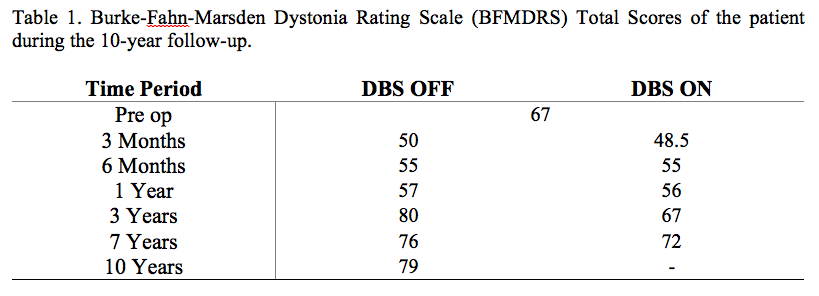
Results: Assessment using the Burke-Fahn-Marsden Dystonia Rating Scale (BFMDRS) throughout his 10-year follow-up initially showed minimal improvement in the dystonic symptoms but it progressively worsened in the successive follow-ups and it did not show any functional significance. [Table1]
Conclusion: Deep brain stimulation using asymmetrical targets in the right and left hemispheres failed to improve the motor symptoms of RDP.
References: [1] Brucke C, Horn A, Huppke P, Kupsch A, Schneider GH and Kuhn A. Failure of pallidal deep brain stimulation in a case of rapid-onset dystonia parkinsonism (DYT12). Movement Disorders Clinical Practice. 2014; 76-78. [2] Dobyns WB, Ozelius LJ, Kramer PL., et al. Rapid-onset dystonia parkinsonism. Neurology. 1993; 43: 2596-2602. [3] Brashear A, Dobyns WB, de Carvalho Aguiar P, et al. The phenotypic spectrum of rapid-onset dystonia parkinsonism (RDP) and mutations in the ATP1A3 gene. Brain 2007; 130:828-835. [4] Deutschlander A, Asmus F, Gasser T, Steude U and Botzel K. Sporadic rapid-onset dystonia parkinsonism syndrome: Failure of bilateral pallidal stimulation. Movement Disorders. 2005; 20:254-257. [5] Fearon C, McKinley J, McCarthy A, et al. Failure of sequential pallidal and motor thalamus DBS for rapid-onset dystonia-parkinsonism (DYT12). Movement Disorders Clinical Practice. 2018; 5:444-445. [6] Fremont R, Calderon DP, Maleki S, Khodakhah K. Abnormal high-frequency burst firing of cerebellar neurons in rapid-onset dystonia parkinsonism. Journal of Neuroscience. 2014; 34:35:11723-11732. [7] Lee JY, Gollamudi S, Ozelius L, Kim JY, and Jeon B. ATP1A3 mutation in the first Asian case of rapid-onset dystonia-parkinsonism. Movement Disorders. 2007; 22: 1808-1809. [8] Sekimoto S, Oyama G, Takayuki J, Hattori N, et al. “Two odd target” strategy in deep brain stimulation for Parkinson’s Disease with unilateral levodopa-induced dystonia. Neurology and Clinical Neuroscience. 2017; 5: 129-130. [9] Weber J, Piroth T, Rijnthes M, Jung B, et al. Atypical presentation of rapid-onset dystonia parkinsonism (DYT12) unresponsive to deep brain stimulation of the subthalamic nucleus. Movement Disorders Clinical Practice. 2018; 5:427-429. [10] Wohrle J, Blahak C, Capelle HH, Fogel W, Bazner H and Krauss J. Combined pallidal and subthalamic nucleus stimulation in sporadic dystonia parkinsonism. Journal of Neurosurgery. 2012; 116: 95-98.
To cite this abstract in AMA style:
J.N Ong, J. Shin, H.J Kim, S.H Paek, B. Jeon. Deep Brain Stimulation using Asymmetrical Targets in Rapid-onset Dystonia Parkinsonism (RDP) [abstract]. Mov Disord. 2020; 35 (suppl 1). https://www.mdsabstracts.org/abstract/deep-brain-stimulation-using-asymmetrical-targets-in-rapid-onset-dystonia-parkinsonism-rdp/. Accessed July 20, 2026.« Back to MDS Virtual Congress 2020
MDS Abstracts - https://www.mdsabstracts.org/abstract/deep-brain-stimulation-using-asymmetrical-targets-in-rapid-onset-dystonia-parkinsonism-rdp/