Category: Dystonia: Clinical Trials and Therapy
Objective: Managing generalized dystonia in adults is challenging despite pharmacological interventions due to suboptimal response or intolerable side effects. While bilateral Globus Pallidus internus Deep Brain Stimulation effectively alleviates dystonic symptoms, limited documentation exists on the benefits of unilateral stimulation. This case report presents successful treatment of generalized dystonia using unilateral GPi-DBS due to suboptimal lead placement.
Background: DBS has replaced unilateral pallidotomy for managing generalized dystonia. Limited evidence exists for unilateral stimulation’s efficacy, but positive results were reported in combining unilateral GPi-DBS with contralateral GPi lesions and unilateral STN stimulation.
Method: We present a 48-year-old female patient, no family history, with progressive generalized dystonia exhibited predominant axial dystonia with marked trunk hyperextension, causing mobility impairment and social withdrawal. Oral medications and botulinum toxin injections were ineffective. She was submitted to bilateral GPI-DBS implantation. Left lead stimulation resulted in side effects, indicating misplacement. We deactivated the left lead and right lead’s parameters were optimized.
Results: Despite unilateral stimulation, the patient experienced remarkable improvements in mobility and overall functionality. Over a six-year follow-up, the patient expressed satisfaction with unchanged therapy. No new neurological complaints were reported. Pre-DBS BFMDRS score was 79/120, improving to 20/120 post-DBS and remaining stable.
Conclusion: The precise impact of unilateral stimulation and potential microlesions on the left GPi is uncertain. Microlesion effects are temporary, suggesting minimal influence on dystonia. Alternatively, motor benefits may persist after DBS interruption, especially in younger patients. The brief period between symptom onset and surgery and the dystonia type likely contributed to the optimal therapeutic unilateral stimulation response. Unilateral GPi-DBS offers advantages such as cost-effectiveness and reduced invasiveness. Randomized controlled studies comparing unilateral and bilateral DBS are still lacking. It could offer a viable option, particularly for patients with prominent axial symptoms or previously submitted to another procedure unilaterally. Finally, it could address challenges faced in regions with limited DBS resources.
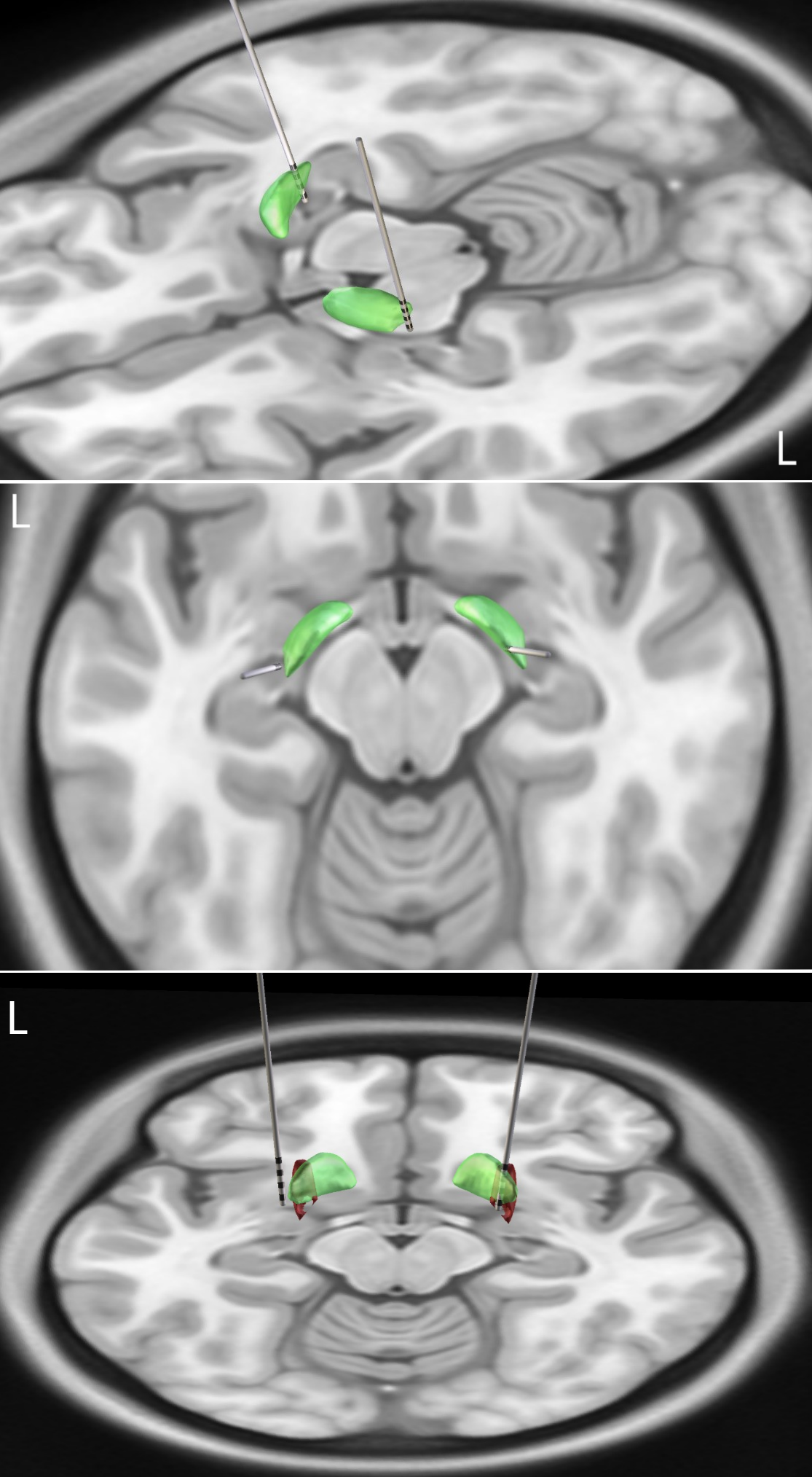
Figure
References: 1. Vidailhet M, Vercueil L, Houeto JL, Krystkowiak P, Benabid AL, Cornu P, et al. Bilateral deep-brain stimulation of the globus pallidus in primary generalized dystonia. N Engl J Med. 2005;352(5):459-467. doi: 10.1056/NEJMoa042187
2. Islekel S, Zileli M, Zileli B. Unilateral pallidal stimulation incervical dystonia. Stereotact Funct Neurosurg 1999;72:248 –252.
3. Page D, Butler A, Jahanshahi M. Quality of life in focal, segmental, and generalized dystonia. Movement disorders: official journal of the Movement Disorder Society. 2007 Feb 15;22(3):341-7.
4. Andy OJ. Thalamic stimulation for control of movement disorders. Appl Neurophysiol 1983;46:107–111.
5. Vercueil L, Pollak P, Fraix V, Caputo E, Moro E, Benazzouz A, Xie J, Koudsie A, Benabid AL. Deep brain stimulation in the treatment of severe dystonia. J Neurol 2001;248:695–700. 6. Loher TJ, Hasdemir MG, Burgunder JM, Krauss JK. Long-term follow-up study of chronic globus pallidus internus stimulation for posttraumatic hemidystonia. Case Report. J Neurosurg 2000;92: 457–460.
7. Cersosimo MG, Raina GB, Piedimonte F, Antico J, Graff P, Micheli FE. Pallidal surgery for the treatment of primary generalized dystonia: long-term follow-up. Clinical neurology and neurosurgery. 2008 Feb 1;110(2):145-50.
8. Vitek JL, Chockkan V, Zhang JY et al. Neuronal activity in the basal ganglia in patients with generalized dystonia and hemiballismus. Ann. Neurol. 46, 22–35 (1999)
9. Chang JW, Choi JY, Lee BW, Kang UJ, Chung SS. Unilateral globus pallidus internus stimulation improves delayed onset post-traumatic cervical dystonia with an ipsilateral focal basal ganglia lesion. J. Neurol. Neurosurg. Psychiatry 73, 588–590 (2002).
10. Tagliati M, Shils J, Sun C, Alterman R. Deep brain stimulation for dystonia. Expert review of medical devices. 2004 Sep 1;1(1):33-41.
11. Cheung T, Zhang C, Rudolph J, Alterman RL, Tagliati M. Sustained relief of generalized dystonia despite prolonged interruption of deep brain stimulation. Movement Disorders. 2013 Sep;28(10):1431-4.
12. Prakash P, Deuschl G, Ozinga S, Mitchell KT, Cheeran B, Larson PS, Merola A, Groppa S, Tomlinson T, Ostrem JL. Benefits and Risks of a Staged‐Bilateral VIM Versus Unilateral VIM DBS for Essential Tremor. Movement Disorders Clinical Practice. 2022 Aug;9(6):775-84.
13. Mitchell KT, Larson P, Starr PA, Okun MS, Wharen Jr RE, Uitti RJ, Guthrie BL, Peichel D, Pahwa R, Walker HC, Foote K. Benefits and risks of unilateral and bilateral ventral intermediate nucleus deep brain stimulation for axial essential tremor symptoms. Parkinsonism & related disorders. 2019 Mar 1;60:126-32.
14. Reich MM, Horn A, Lange F, Roothans J, Paschen S, Runge J, Wodarg F, Pozzi NG, Witt K, Nickl RC, Soussand L. Probabilistic mapping of the antidystonic effect of pallidal neurostimulation: a multicentre imaging study. Brain. 2019 May 1;142(5):1386-98.
15. Kupsch A, Benecke R, Muller J, Trottenberg T, Schneider GH, Poewe W, et al. Pallidal deep-brain stimulation in primary generalized or segmental dystonia. N Engl J Med 2006; 355: 1978–90.
16. Volkmann J, Wolters A, Kupsch A, Muller J, Kuhn AA, Schneider GH, et al. Pallidal deep brain stimulation in patients with primary generalised or segmental dystonia: 5-year follow-up of a randomised trial. Lancet Neurol 2012; 11: 1029–38.
17. Walsh RA, Sidiropoulos C, Lozano AM, Hodaie M, Poon YY, Fallis M, et al. Bilateral pallidal stimulation in cervical dystonia: blinded evidence of benefit beyond 5 years. Brain 2013; 136 (Pt 3): 761–9.
To cite this abstract in AMA style:
K. Massruha, I. Brum, C. Listik, J. Yamamoto, S. Casagrande, M. Belo Silva, P. Medeiros Lacerda, V. Zanesi Maciel, R. Cury, E. Barbosa. Effective Management of Generalized Dystonia with Unilateral Deep Brain Stimulation – Killing Two Birds with One Stone? [abstract]. Mov Disord. 2024; 39 (suppl 1). https://www.mdsabstracts.org/abstract/effective-management-of-generalized-dystonia-with-unilateral-deep-brain-stimulation-killing-two-birds-with-one-stone/. Accessed August 4, 2026.« Back to 2024 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/effective-management-of-generalized-dystonia-with-unilateral-deep-brain-stimulation-killing-two-birds-with-one-stone/