Objective: To evaluate the cause of unsteadiness in 4 patients with segmental dystonia
Background: Mild impairment of postural control has been described in focal and segmental, especially cervical dystonia (1). Slow orthostatic tremor (OT) with dystonia and OT plus can also be responsible for postural instability. A retrospective series of 93 patients with unexplained unsteadiness had 16 (17.2%) patients with orthostatic myoclonus (OM), 13.9% with OT and 12.9 % with slow OT (2). OM, combined with dystonia as a cause of instability has not been previously described.
Method: 4 patients with segmental dystonia sparing lower limbs were evaluated for unsteadiness. Brain imaging and nerve conduction studies ruled out secondary or peripheral causes of instability. Tremor study with surface EMG of lower limbs (bilateral gastrocnemius, tibialis anterior (TA), quadriceps, hamstrings) was done in all except case 1.
Results: Case 1- 58 year-old gentleman presented with unsteadiness while standing and walking from 3-4 months. No slowness, cognitive or autonomic complaints. Sister also had similar complaints. Examination – mild bi-brachial dystonia, palpable tremor on standing in bilateral gastrocnemius, TA, hamstrings, quadriceps. Patient did not tolerate Clonazepam, but responded to Pacitane with no instability or palpable tremor on follow-up.
Case 2- (sibling of case 1)- 72 year-old lady with 10 yrs duration of unsteadiness while standing and walking, mild tremors in hands. She had mild laterocollis with dystonia of fingers with postural tremors in hands, no lower limb palpable tremors. Rest normal neurological examination. Tremor study showed 4-5 Hz orthostatic myoclonus (Figure 1). Responded well to Clonazepam.
Case 3- 72 year-old gentleman with unsteadiness while standing and walking and tremulousness of legs from 2 years, needing support to walk now. Examination- bilateral hand dystonia with dystonic tremor and palpable tremor in legs. Tremor study showed 8-9 Hz orthostatic myoclonus (Figure 2). No good response to Clonazepam.
Case 4- A 70 year-old gentleman with unsteadiness while walking from 3-4 years and tremulousness of hands while writing. Examination – mild bibrachial dystonia. Tremor study- 13-14 Hz orthostatic tremor (Figure 3). Responded to Clonazepam.
Conclusion: Orthostatic myoclonus can be a cause of unexplained instability in patients with mild segmental dystonia and should be looked for during clinical examination and with surface EMG.
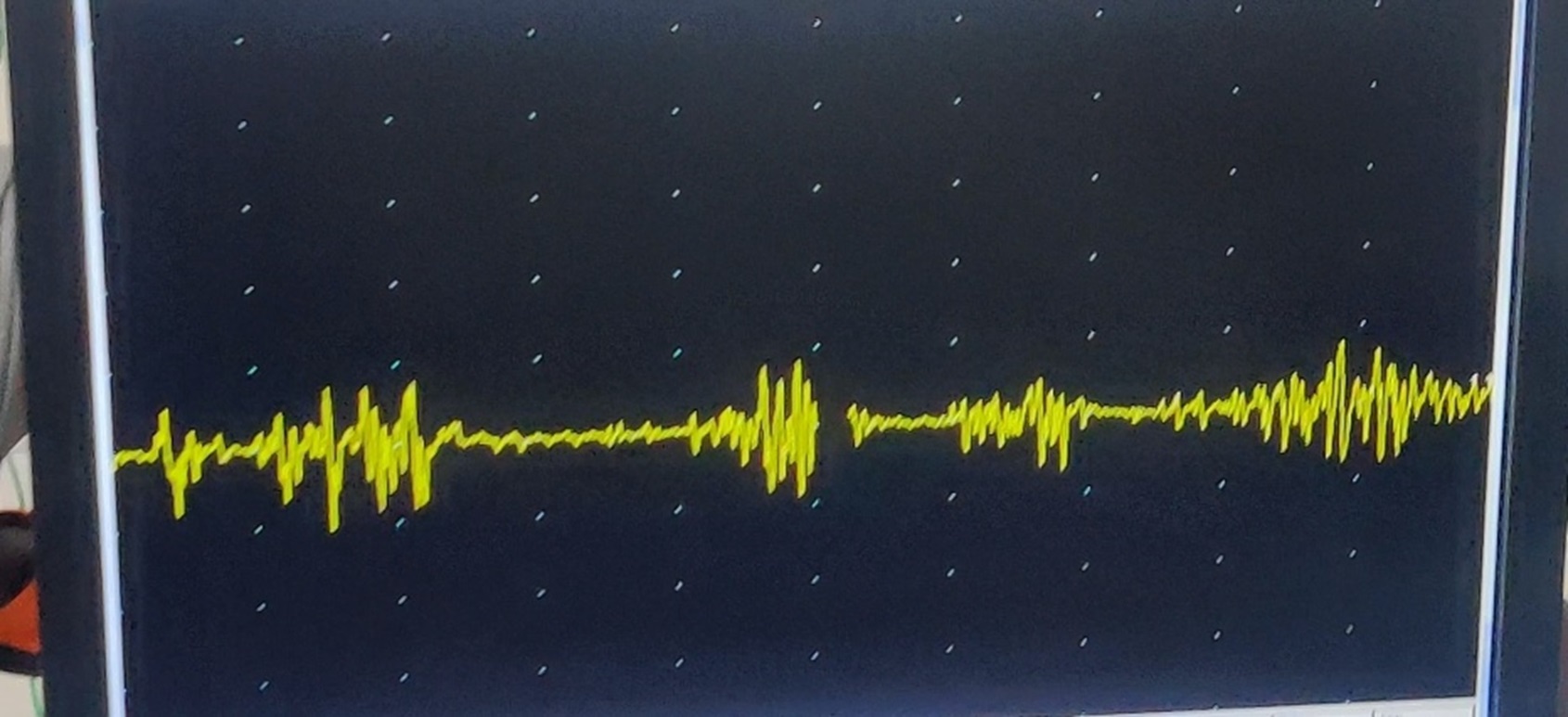
Figure 1
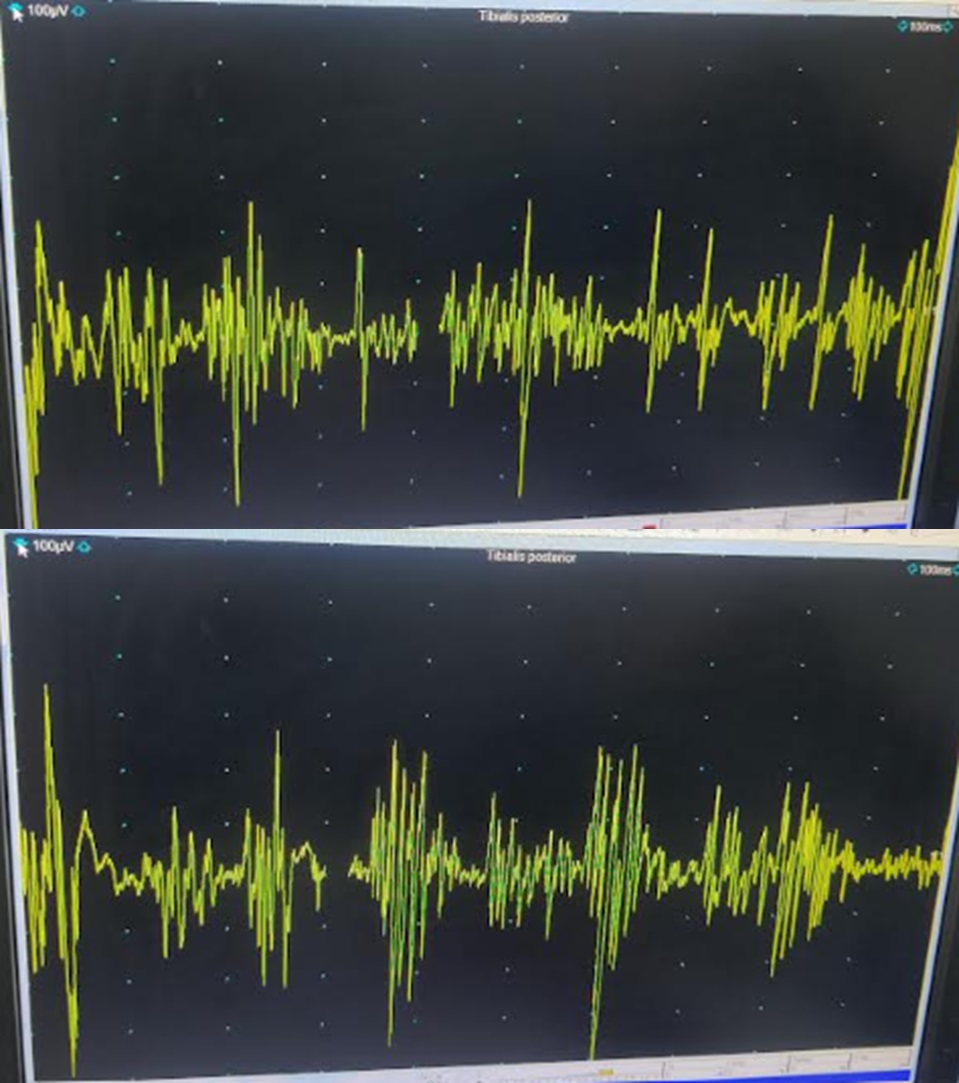
Figure 2
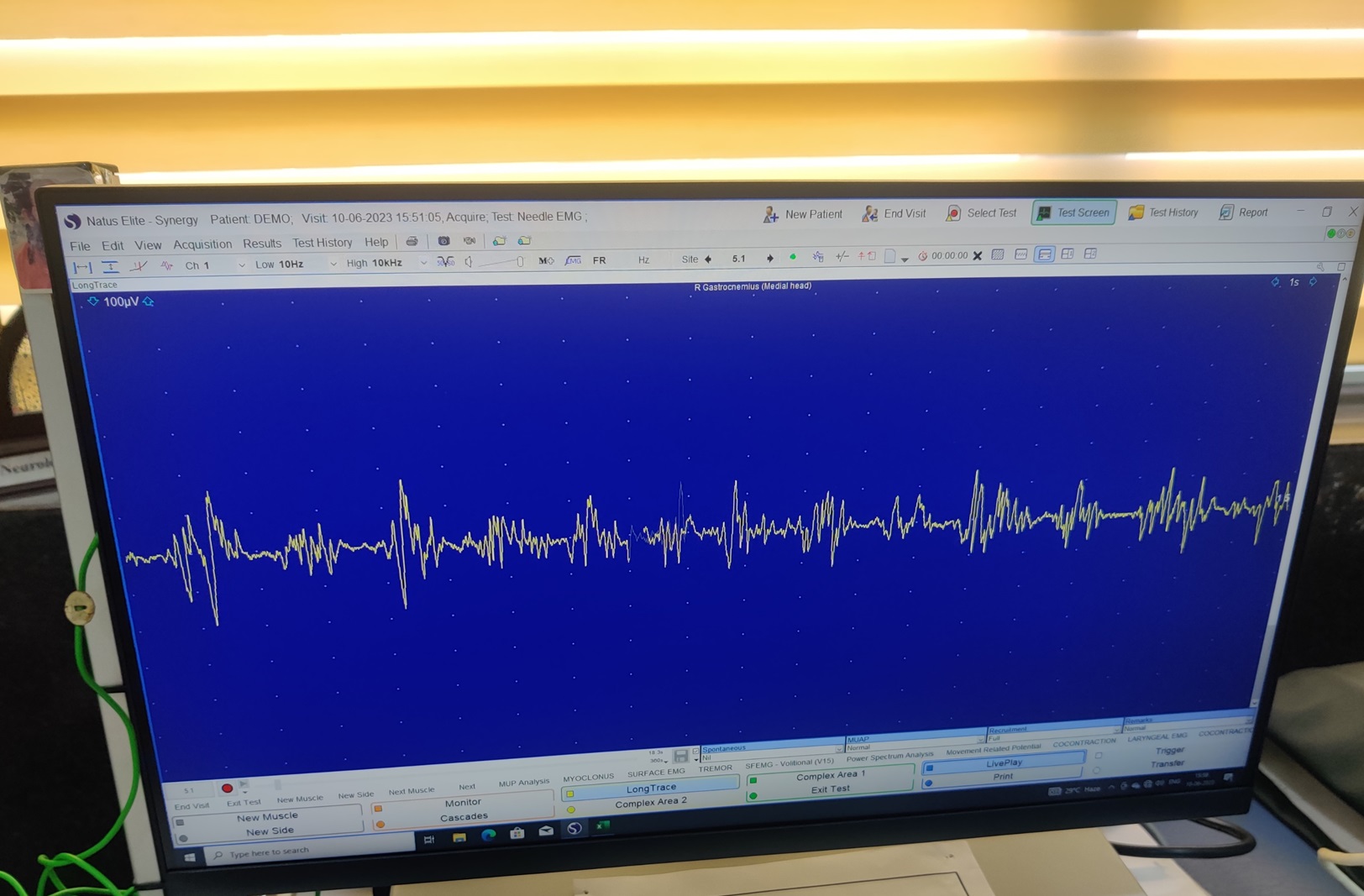
FIgure 3
References: 1. Esposito M, Dubbioso R, Peluso S, et al. Cervical dystonia patients display subclinical gait changes. Parkinsonism Relat Disord. 2017;43:97-100. doi:10.1016/j.parkreldis.2017.07.005
2. Gasca-Salas C, Arcocha J, Artieda J, Pastor P. Orthostatic myoclonus: an underrecognized cause of unsteadiness? Parkinsonism Relat Disord. 2013;19(11):1013-1017. doi:10.1016/j.parkreldis.2013.07.004
To cite this abstract in AMA style:
K. Pillai, P. Chavan, K. Mansukhani, V. Patil, A. Sharma, H. Halani, V. Pardasani, S. Khadilkar, J. Lalkaka, R. Singh, N. Barucha. Evaluation of unsteadiness in patients with dystonia [abstract]. Mov Disord. 2024; 39 (suppl 1). https://www.mdsabstracts.org/abstract/evaluation-of-unsteadiness-in-patients-with-dystonia/. Accessed August 8, 2026.« Back to 2024 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/evaluation-of-unsteadiness-in-patients-with-dystonia/