Category: Parkinson's Disease: Surgical Therapy
Objective: To compare 3 methods of localising STN DBS programs for PD; 1) clinical standard of care (SOC), 2) imaging-based programming (IBP), 3) novel algorithm using evoked resonant neural activity (ERNA).
Background: Clinical heuristic STN-DBS programming in PD yields variable outcomes.1 Imaging-guided platforms offer objective guidance to localise stimulation. ERNA recorded intraoperatively also has programming utility.2,3 We investigated differences in current fractionation montages derived by these methods.
Method: 42 subjects with STN DBS for PD (79 leads) were enrolled in an observational study (Table1). We compared 3 programs:
SOC: Optimised over 4 months by a high-volume DBS team
EBP (ERNA-based programming): Current apportioned by a computer algorithm according to distribution of ERNA power across electrodes on 2 adjacent tiers
IBP: Commercial software with automated lead localisation. An expert clinician generated electrical fields targeting the dorsal STN and derived current apportionment.
For each program, centre-of-mass (CoM) was derived from the weighted mid-point of fractionated current across electrodes.
Outcomes:
Longitudinal offset: Distance of CoM along the lead axis compared to mid-point [Fig1a].
Radial offset: Angle of direction of CoM compared to anterior orientation in a plane 90° to lead axis. Left STN CoM were mirrored in the med-lat plane for directional analysis [Fig1b].
Kruskal-Wallis test assessed differences in axial offset. Conover test adjusted by Holm method analysed pairwise differences. Watson-Wheeler test compared radial offsets.
Results: Longitudinal offset significantly differed between conditions (H(2)=98.3, p<0.001). EBP stimulated 1.2mm ventral to SOC (median [IQR] -0.4mm [0.8] vs 0.8 [0.8], p<0.001) and IBP (0.8 [0.8], p<0.001) [Fig2]. Radial offsets were compared for 19 leads that used directional programs for all conditions. There was no significant difference between conditions (mean [SD] EBP 73.8° [42.5], SOC 58.8 [82.9], IBP 45.4 [60.0], W(4)=8.9, p=0.06). EBP radial offsets showed a lateral trend compared to SOC (p=0.07) [Fig3].
Conclusion: Current fractionation guided by an ERNA algorithm localised stimulation more ventrally along the lead axis than SOC and IBP. As 1.2mm is 80% of an electrode, it is likely to be clinically relevant. Whether this is a consistent finding requiring offsets in future algorithms is being studied.
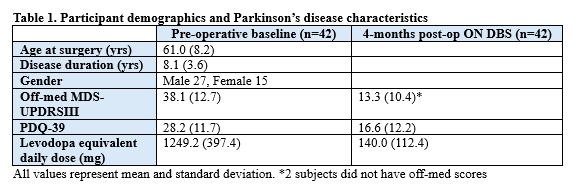
Table 1
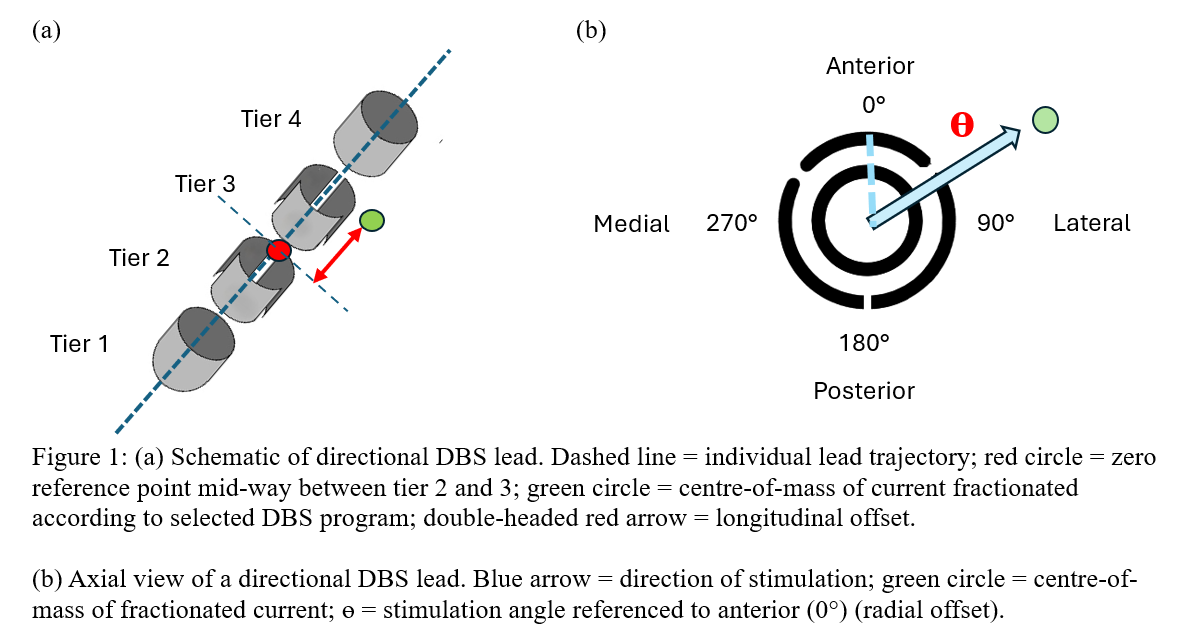
Figure 1
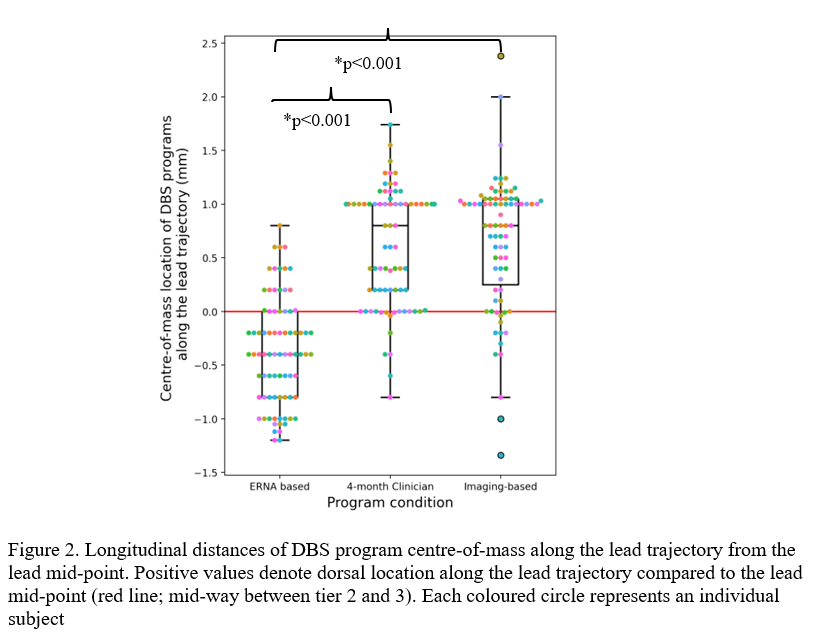
Figure 2
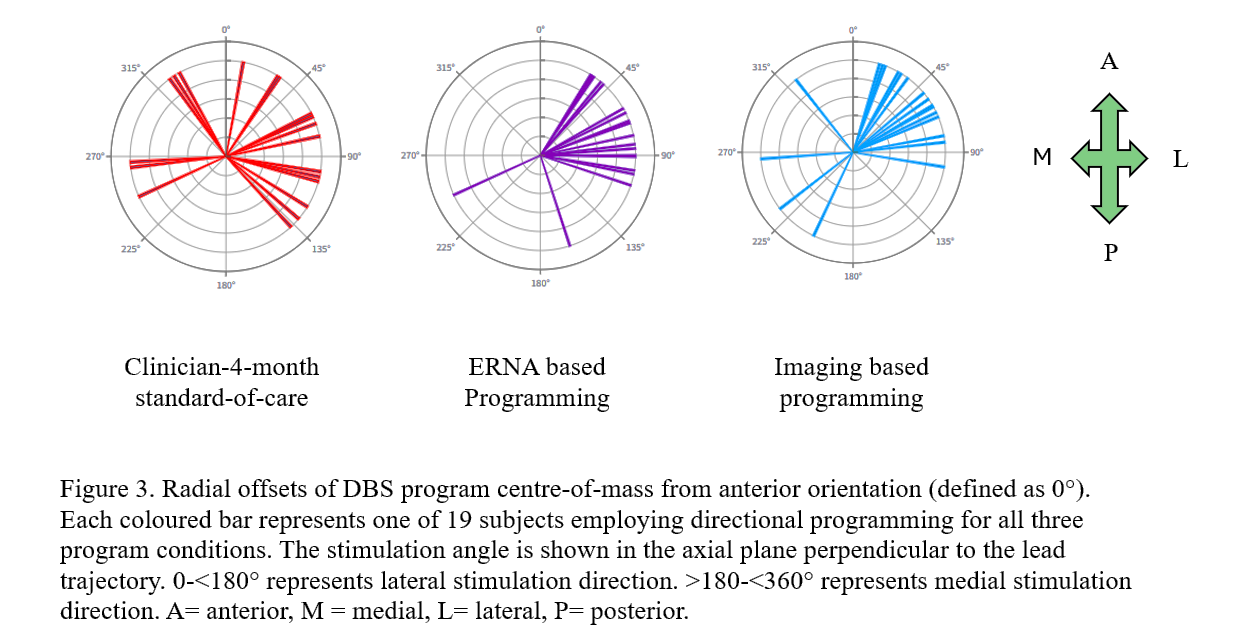
Figure 3
References: 1. Okun MS, Tagliati M, Pourfar M, et al. Management of Referred Deep Brain Stimulation Failures: A Retrospective Analysis From 2 Movement Disorders Centers. Arch Neurol. 2005;62(8):1250. doi:10.1001/archneur.62.8.noc40425
2. Xu SS, Sinclair NC, Bulluss KJ, et al. Towards guided and automated programming of subthalamic area stimulation in Parkinson’s disease. Brain Communications. 2022;4(1):fcac003. doi:10.1093/braincomms/fcac003
3. Nagao K, Perera T, Petoe M, et al. Evoked Resonant Neural Activity Automates Field Shaping of Subthalamic Nucleus-Deep Brain Stimulation in Parkinson’s Disease [abstract]. Mov Disord. 2024; 39 (suppl 1). https://www.mdsabstracts.org/abstract/evoked-resonant-neural-activity-automates-field-shaping-of-subthalamic-nucleus-deep-brain-stimulation-in-parkinsons-disease/.
To cite this abstract in AMA style:
K. Nagao, T. Perera, M. Petoe, W-L. Lee, H. Mcdermott, K. Bulluss, W. Thevathasan. Evoked Resonant Neural Activity localises STN DBS programs more ventrally than clinician and imaging-guided methods in Parkinson’s disease [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/evoked-resonant-neural-activity-localises-stn-dbs-programs-more-ventrally-than-clinician-and-imaging-guided-methods-in-parkinsons-disease/. Accessed April 9, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/evoked-resonant-neural-activity-localises-stn-dbs-programs-more-ventrally-than-clinician-and-imaging-guided-methods-in-parkinsons-disease/