Session Information
Date: Sunday, October 7, 2018
Session Title: Dystonia
Session Time: 1:45pm-3:15pm
Location: Hall 3FG
Objective: To evaluate the role of radiosurgical thalamotomy in cases of medically refractory generalised dystonia in current era.
Background: Gamma knife radiosurgery has been proved to be effective in the management of medically refractory dystonia. Technically, it is considered inferior to deep brain stimulation on the virtue of absence of real time monitoring, latency period for effective results, and irreversible nature of lesioning [1]. We present our experience with five cases of generalised dystonia managed with radiosurgery ablation of the posteroventral thalamic nuclei.
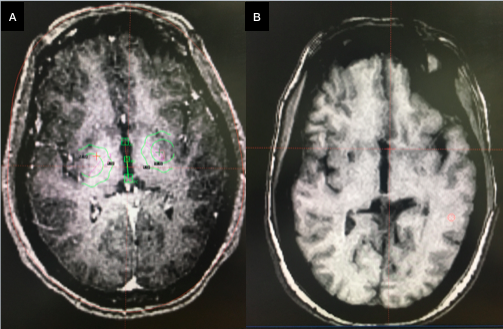
Methods: 5 patients were treated with Leksell Perfexion gamma knife radiosurgery. 3/5 patients were primary dystonia, while one was suffering from neuroacanthosis, and another developed post traumatic dystonia. The lesion was created at bilateral posteroventral thalamic nucleus. The target was localised on magnetic resonance imaging after fusion with anatomical atlas. A single shot of 4 mm collimator was used with 140 Gy marginal dose at prescription iso dose of 100% [1,2]. Peri procedure steroids were administered.
Results: The median time to improvement was 70 days. Complete abolition of movement was observed in 20% of patients, while excellent relief in 40%. New onset deficit was observed in 2/5 (40%) patients. One patient developed bilateral homonymous hemianopia within one week of GKRS. Another patient developed hemiparesis after 4 months of radiosurgery due to development of infarct in the posterior limb of internal capsule. One patient developed steroid resistant brain edema which needed Bevacizumab for the management. Follow up radiology at three months resulted in 4-5 mm well circumscribed lesion with peripheral contrast enhancement surrounding a low signal region.
Conclusions: Radiosurgical thalamotomy is not a shot in the dark. Posteroventral thalamotomy should still be considered a treatment modality for selected cases of dystonia. It remains an attractive option in patients with advanced age, significant medical comorbidities, that forbid open stereotactic procedures, or patients on anticoagulation therapy. In resource stricken countries such as India, where majority of the population remains noninsured, lesion intervention is a more feasible option.
References: Krack P et al. Current applications and limitations of surgical treatments for movement disorders. Mov Disord 2017;32:36-52. Bereau M, Tranchant C. Movement Disorders: An Update. Rev Med Interne 2017. doi:10.1016/j.revmed.2017.09.001.
To cite this abstract in AMA style:
M. Tripathi. Gamma Knife Radiosurgery for Generalised Dystonia: Is It The Last Part in The Ship of Theseus [abstract]. Mov Disord. 2018; 33 (suppl 2). https://www.mdsabstracts.org/abstract/gamma-knife-radiosurgery-for-generalised-dystonia-is-it-the-last-part-in-the-ship-of-theseus/. Accessed August 9, 2026.« Back to 2018 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/gamma-knife-radiosurgery-for-generalised-dystonia-is-it-the-last-part-in-the-ship-of-theseus/