Category: Non-Dystonia (Other)
Objective: To report a case of hemiballism as a previously unreported complication of MRI-guided focused ultrasound (MRgFUS) thalamotomy for essential tremor (ET).
Background: MRgFUS of the ventral intermediate (VIM) nucleus is an FDA approved therapy for refractory ET, offering a less invasive alternative to conventional thalamotomy. It provides sustained tremor relief, with transient paresthesia and gait ataxia as common side effects. Hemichorea and ballism have not been previously described following VIM thalamotomy for ET.
Method: Case report.
Results: An 87-year-old right-handed female with atrial fibrillation on apixaban and longstanding ET developed involuntary right arm movement three weeks after left VIM MRgFUS thalamotomy for medication-refractory tremor at an outside academic center. Anticoagulation was held preoperatively and resumed two days post-procedure. She had immediate tremor relief and transient gait ataxia, with post-operative MRI showing an appropriate lesion in the left VIM with surrounding edema.
However, she developed high-amplitude right arm greater than leg movements in conjunction with a fall three weeks post procedure. A repeat MRI at three months showed new susceptibility within the left VIM lesion indicative of micro hemorrhage extending laterally toward the posterior limb of the left internal capsule and inferiorly toward the midbrain [Figure 1]. Multiple pharmacologic agents, including amantadine, propranolol, and VMAT-2 inhibitors, were ineffective or poorly tolerated.
One-year post-procedure, she presented to our clinic with disabling ballistic right arm movements, motor persistence, and impaired ambulation due to significant retro flailing. Ultrasound and electromyography-guided botulinum toxin injection to the involved musculature [Table 1] resulted in 50% reduction in the amplitude of her right arm ballistic movements without weakness, leading to improved functional control and independent ambulation.
Conclusion: This is, to our knowledge, the first reported case of hemiballism as a presumed complication of MRgFUS VIM thalamotomy for ET. Imaging suggests spontaneous hemorrhage within the VIM lesion upon restarting anticoagulation, affecting the subthalamic nucleus leading to ballism. The optimal timing of resuming anticoagulation remains unclear. Botulinum toxin injections may be an effective option for refractory hemiballism.
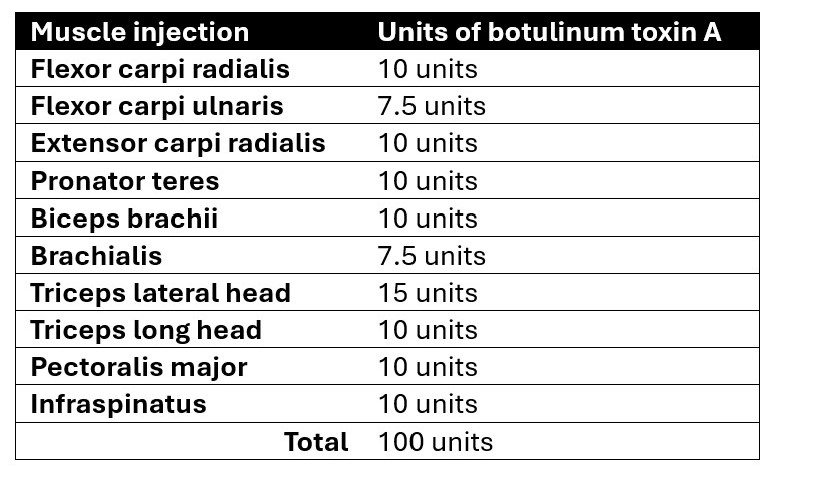
Table 1: Botulinum toxin regimen
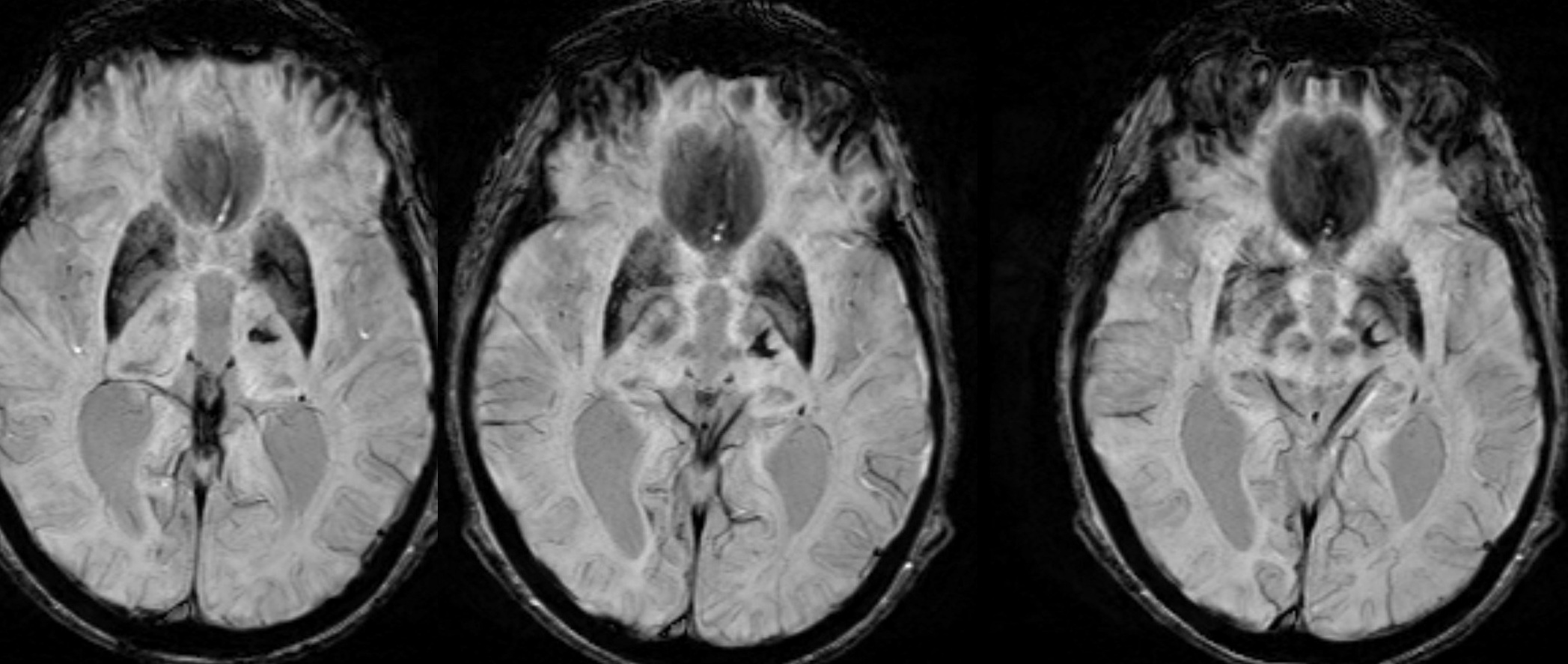
Figure 1: Axial MRI SWI sequence
To cite this abstract in AMA style:
M. Govil, N. Beltre, P. Drummond. Hemiballism after MRI guided focused ultrasound thalamotomy for essential tremor [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/hemiballism-after-mri-guided-focused-ultrasound-thalamotomy-for-essential-tremor/. Accessed April 10, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/hemiballism-after-mri-guided-focused-ultrasound-thalamotomy-for-essential-tremor/