Category: Other
Objective: To evaluate the clinical characteristics, etiologies, treatment, and evolution of patients with immune-mediated movement disorders(IMMD).
Background: The highly variable and complex phenomenology of IMMD and the increasing number of related autoantibodies being described significantly hinder its diagnosis. At this moment, IMMD prevalence is unknown. Since these diseases are potentially treatable and can be associated with several occult neoplasms, early diagnosis may be crucial to modify its prognosis.
Method: We performed a multicenter, retrospective, and descriptive case series.Thirteen centers from Argentina participated(period analyzed: 2008-2020).Patients had to be ≥15 years-old. To be included, the movement disorder(MD)had to be associated with a potentially pathogenic antibody according to the literature,or occur in the context of a typical paraneoplastic syndrome with no identified antibody but associated with a cancer diagnosis in the previous five years, or present without antibodies or associated cancer but with an exceptional response to immunosuppressants(≥ 90%)and no other better explanation. Clinical syndromes were divided into hyperkinetic or hypokinetic. We assessed differences according to age(≤50 vs >50 years).
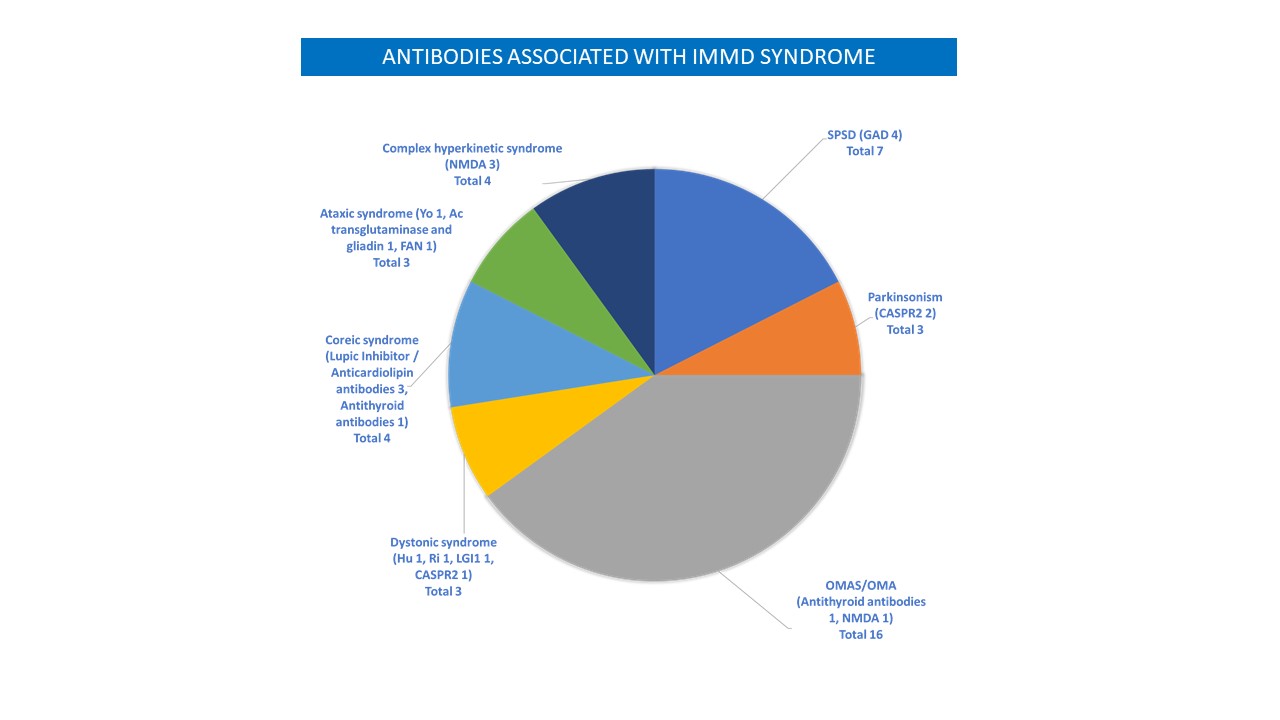
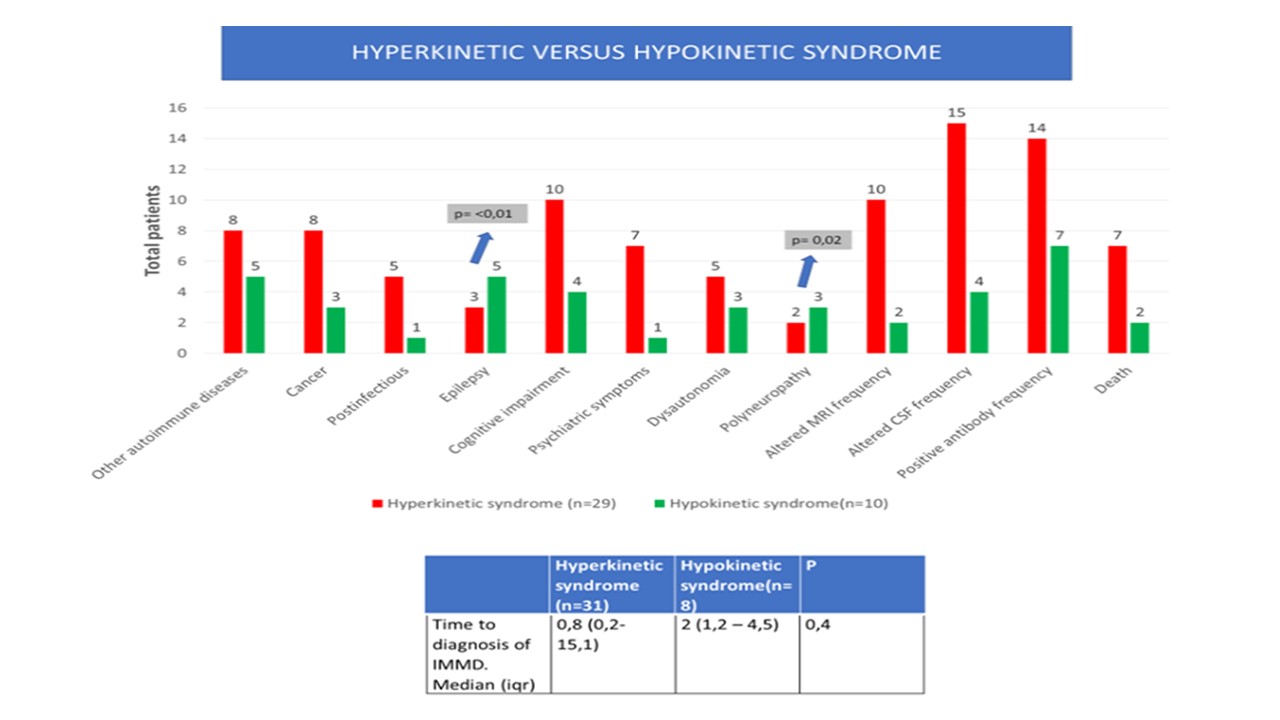
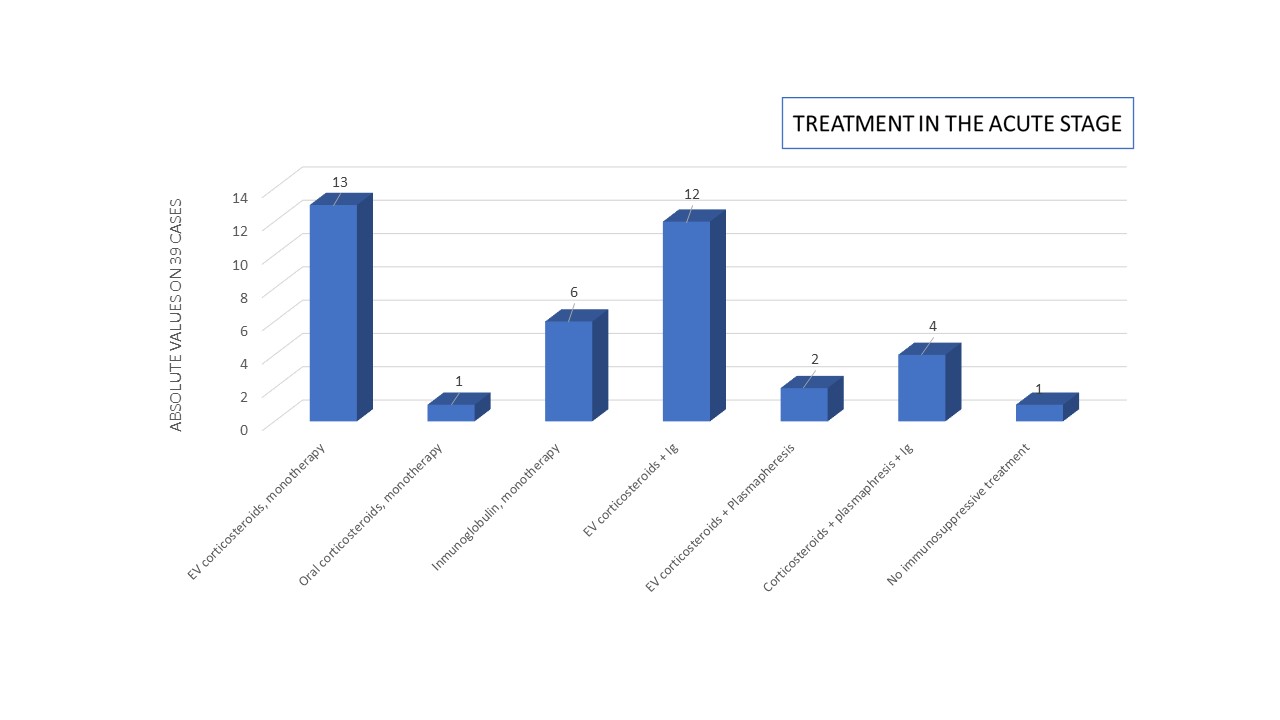
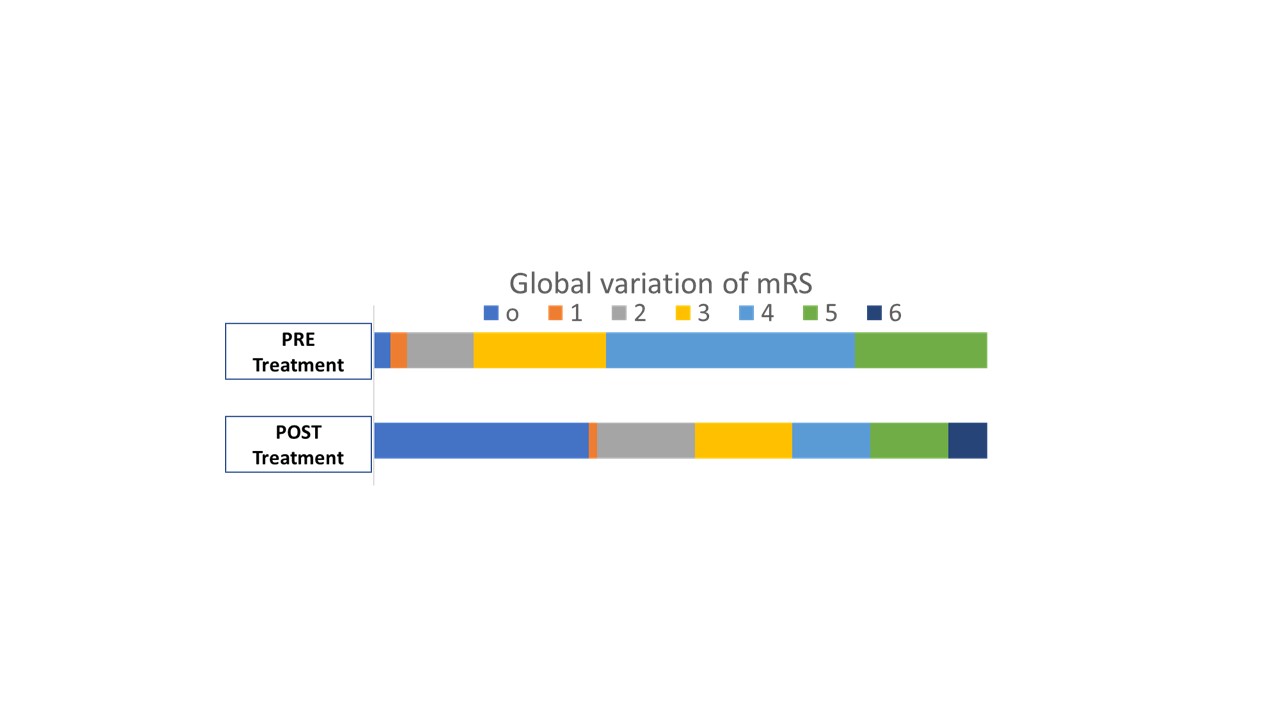
Results: Thirty-nine patients were included (female:23). Mean age (SD): 51.5 (18.8); ≤50 years: 43.6%. Acute/subacute clinical presentation:67%. Hyperkinetic syndromes (79.6%)and generalized forms(69.2%)were more frequent. We found an association with cancer in 28.2%. Pathological brain MRI:30.8%, pathological CSF: 48.7%, positive autoantibodies: 53.8%, most frequent treatment: intravenous corticosteroids. Variation of the modified Rankin scale before and after treatment: p<0.01. Nine patients died (7 were>50 years). Hypokinetic syndromes: more frequent in >50 years, higher prevalence of cancer and relapse of the IMMD, greater delay in diagnosis; epilepsy and polyneuropathy were more frequent. Hyperkinetic syndromes: higher prevalence of pathological CSF and brain MRI.
Conclusion: The diagnosis of an IMMD should be considered when symptoms present an acute or subacute onset, are associated with other neurological manifestations, autoimmune diseases and/or cancer, and with a pathological CSF. A substantial percentage of our sample presented positive autoantibodies. We observed a delay in the diagnosis of hypokinetic syndromes. Patients >50 years had a worse prognosis.
To cite this abstract in AMA style:
M. Bala, F. Gonzalez, M. Saucedo, L. Bandeo, A. Chertcoff, L. de Francesco, G. Napoli, L. Leon Cejas, P. Bonardo, N. Morera, L. Tschopp, C. Rugilo, C. Calandra, A. Pellene, G. Raina, Z. Salazar, G. Rinaldi, P. Judewicz, J. Rivas, J. Gustavo Jose, D. Ballesteros, M. Tela, F. Gualtieri, J. Amor, C. Esliman, F. Caiza Zambrano, T. Arakaki, N. Garretto, S. Rodriguez, A. Kohler, A. Laffue, O. Martinez, M. Fernandez Pardal, R. Reisin, C. Uribe Roca. IMMUNE-MEDIATED MOVEMENT DISORDERS: CLINICAL MANIFESTATIONS, TREATMENT, AND EVOLUTION. A MULTICENTER STUDY [abstract]. Mov Disord. 2021; 36 (suppl 1). https://www.mdsabstracts.org/abstract/immune-mediated-movement-disorders-clinical-manifestations-treatment-and-evolution-a-multicenter-study/. Accessed August 3, 2026.« Back to MDS Virtual Congress 2021
MDS Abstracts - https://www.mdsabstracts.org/abstract/immune-mediated-movement-disorders-clinical-manifestations-treatment-and-evolution-a-multicenter-study/