Category: Parkinson’s Disease: Clinical Trials
Objective: To evaluate the effect of foslevodopa/foscarbidopa (LDP/CDP, ABBV-951) on clinical and patient-reported outcomes in advanced Parkinson’s disease (aPD) patients using minimal clinically important difference (MCID) thresholds.
Background: The 24-hr/day continuous subcutaneous infusion of LDP/CDP has demonstrated efficacy in controlling motor fluctuations among patients with aPD in Phase 3 clinical trials. Responder analysis using MCIDs, the smallest change in outcome that is clinically relevant, may facilitate interpretation of treatment effects meaningful to patients [1].
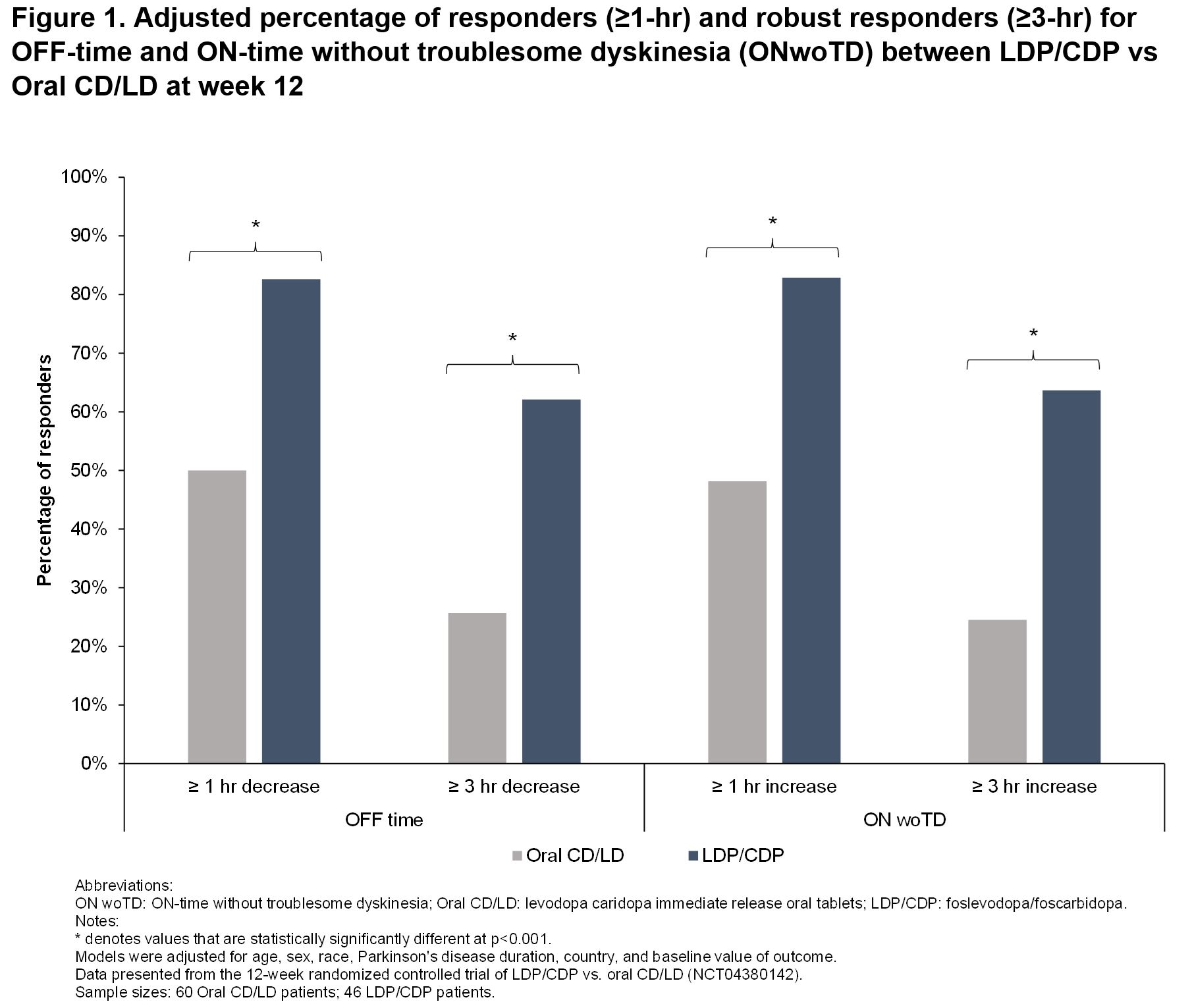
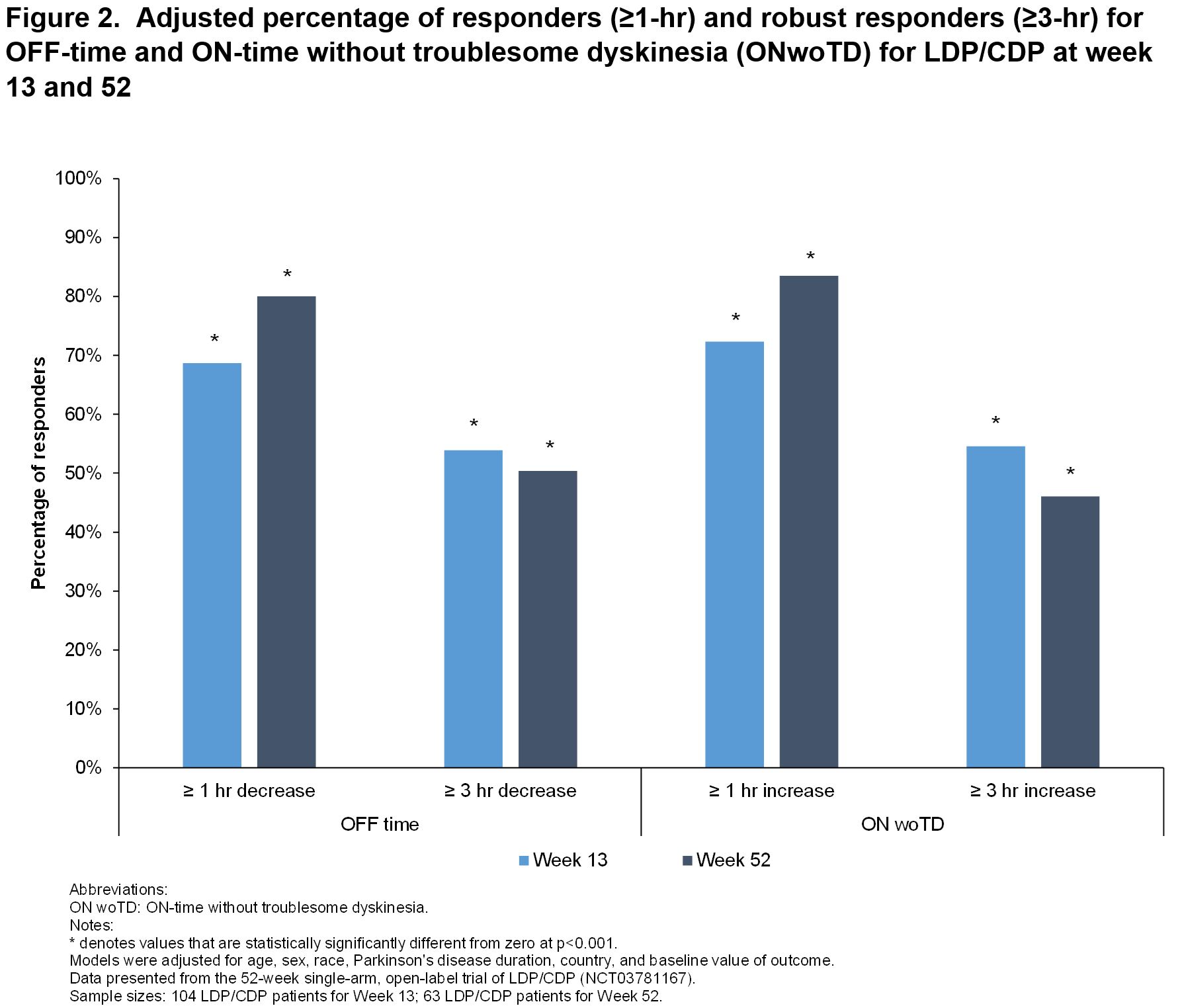
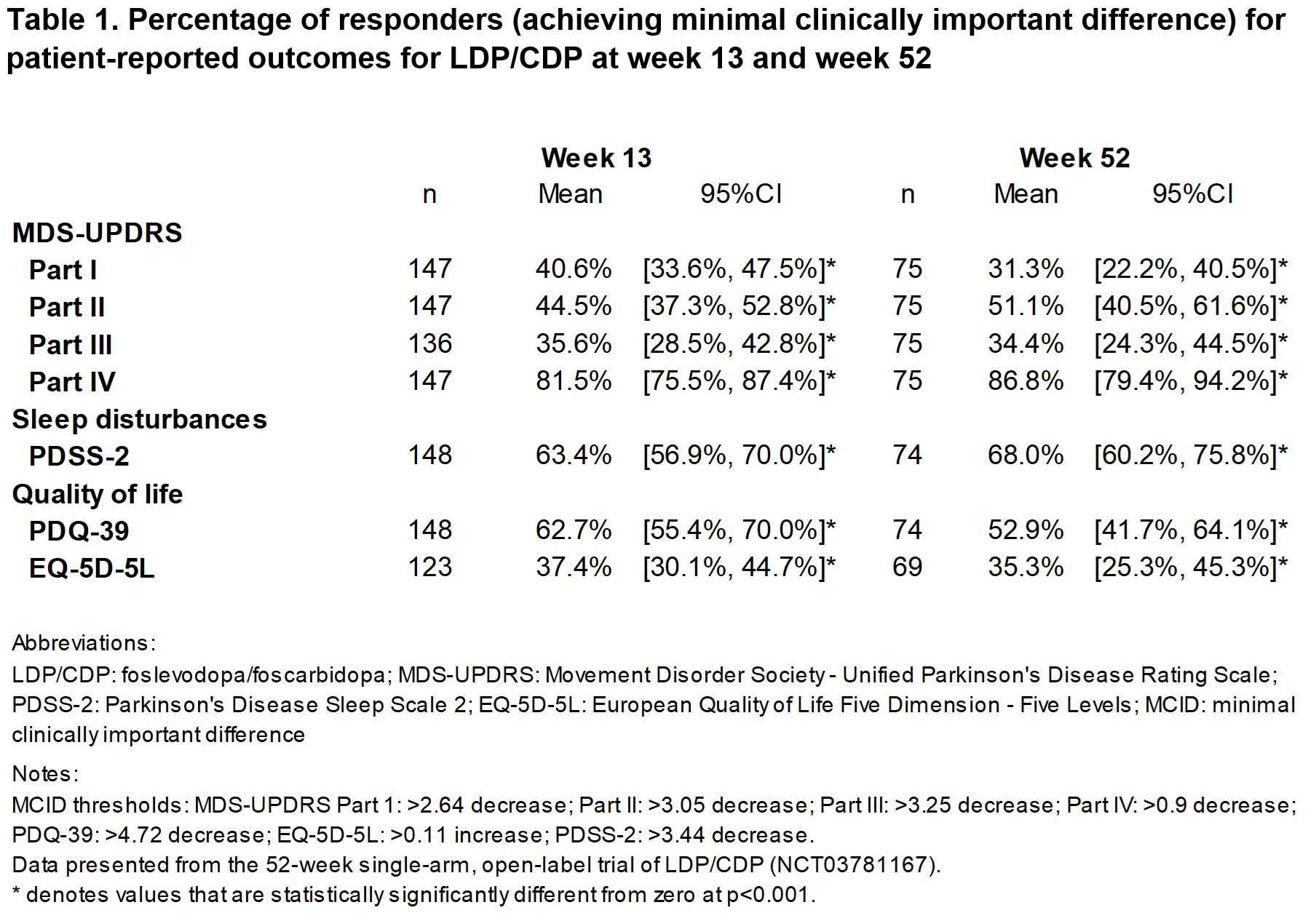
Method: Post-hoc analyses of data from a 12-week (W) randomized controlled trial (RCT) of LDP/CDP vs. oral carbidopa/levodopa (CD/LD) (NCT04380142) and a 52-W single-arm, open-label trial of LDP/CDP (NCT03781167). Responders were identified relative to baseline for increased ON-time without troublesome dyskinesia (ONwoTD, ‘good ON-time’) and reduced OFF-time using a threshold of ≥1-hr and ≥3-hr (robust responder) [2-3]. Established MCIDs were used to evaluate responders for MDS-UPDRS Parts I–IV [4-6], quality of life (QoL; PDQ-39 [7], EQ-5D-5L [8]) and sleep disturbances (PDSS-2 [5]). Adjusted generalized linear models compared responder proportions between LDP/CDP (n=46) vs. CD/LD (n=60) at W12, and for LDP/CDP at W13 (n=148) and W52 (n=75) vs. baseline.
Results: At W12 in the RCT, higher proportions of LDP/CDP vs. CD/LD patients had ≥1-hr (82.6% vs. 50.0%) and ≥3-hour (62.1% vs. 25.7%) reductions in OFF-time, and ≥1-hr (82.9% vs. 48.1%) and ≥3-hr (63.6% vs. 24.5%) increases in ONwoTD (all p<0.001; Fig 1). Response rates were higher in LDP/CDP vs. CD/LD for MDS-UPDRS Parts II (activities in daily living [ADL], 47.0% vs. 21.4%) and IV (motor complications, 60.7% vs. 39.5%), and PDSS-2 (71.5% vs. 42.6%) (all p<0.05). Similar findings were observed in the single-arm, open-label trial for LDP/CDP which demonstrated early (W13) and sustained response (up to W52) in improvements of OFF-time, ONwoTD, ADL, motor complication, QoL, and sleep disturbances (all p<0.001; Fig 2 and Table 1).
Conclusion: Greater proportions of patients on LDP/CDP vs. CD/LD achieved clinically meaningful improvements in OFF-time, ONwoTD, ADL, motor complication, QoL and sleep disturbances. These improvements were seen early and sustained consistently up to W52.
References: [1] McGlothlin AE, Lewis RJ. Minimal clinically important difference: defining what really matters to patients. Jama. 2014 Oct 1;312(13):1342-3.
[2] Elmer, Lawrence W et al. “Pooled Analyses of Phase III Studies of ADS-5102 (Amantadine) Extended-Release Capsules for Dyskinesia in Parkinson’s Disease.” CNS drugs vol. 32,4 (2018): 387-398. doi:10.1007/s40263-018-0498-4.
[3] Zhang, Z. X., Liu, C. F., Tao, E. X., Shao, M., Liu, Y. M., Wang, J., … & Bauer, L. (2017). Rotigotine transdermal patch in Chinese patients with advanced Parkinson’s disease: A randomized, double-blind, placebo-controlled pivotal study. Parkinsonism & related disorders, 44, 6-12.
[4] Horváth K, Aschermann Z, Kovács M, Makkos A, Harmat M, Janszky J, Komoly S, Karádi K, Kovács N. Minimal clinically important differences for the experiences of daily living parts of movement disorder society-sponsored unified Parkinson’s disease rating scale. Mov Disord. 2017 May;32(5):789-793. doi: 10.1002/mds.26960. Epub 2017 Feb 20. PMID: 28218413.
[5] Horváth K, Aschermann Z, Ács P, Deli G, Janszky J, Komoly S, Balázs É, Takács K, Karádi K, Kovács N. Minimal clinically important difference on the Motor Examination part of MDS-UPDRS. Parkinsonism Relat Disord. 2015 Dec;21(12):1421-6. doi: 10.1016/j.parkreldis.2015.10.006. Epub 2015 Oct 22. PMID: 26578041.
[6] Makkos A, Kovács M, Pintér D, Janszky J, Kovács N. Minimal clinically important difference for the historic parts of the Unified Dyskinesia Rating Scale. Parkinsonism Relat Disord. 2019 Jan;58:79-82. doi: 10.1016/j.parkreldis.2018.08.018. Epub 2018 Aug 26. PMID: 30174275.
[7] Horváth K, et al. (2017). Changes in quality of life in Parkinson’s disease: how large must they be to be relevant? Neuroepidemiology, 48(1-2), 1-8.
[8] Winter Y, Lubbe D, Oertel W, Dodel R. Evaluation of minimal clinically important differences for health-related quality of life scales in Parkinson’s Disease. Value in Health. 2012 Nov;15(7):PA279.
To cite this abstract in AMA style:
M. Soileau, J. Aldred, A. Antonini, C. Carroll, V. Fung, T. Henriksen, R. Pahwa, D. Santos Garcia, A. Epstein, C. Yan, A. Alobaidi, A. Shewale, A. Spiegel, M. Facheris, J. Zamudio, P. Kukreja, KR. Chaudhuri. Impact of foslevodopa/foscarbidopa on key clinical and patient-reported outcomes in patients with aPD: Responder analysis of two Phase 3 clinical trials [abstract]. Mov Disord. 2022; 37 (suppl 2). https://www.mdsabstracts.org/abstract/impact-of-foslevodopa-foscarbidopa-on-key-clinical-and-patient-reported-outcomes-in-patients-with-apd-responder-analysis-of-two-phase-3-clinical-trials/. Accessed July 4, 2026.« Back to 2022 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/impact-of-foslevodopa-foscarbidopa-on-key-clinical-and-patient-reported-outcomes-in-patients-with-apd-responder-analysis-of-two-phase-3-clinical-trials/