Category: Myoclonus/Tics/Stereotypies
Objective: To present a case of oculopalatal myoclonus (OPM) secondary to brainstem hemorrhage.
Background: OPM is an acquired syndrome characterized by synchronized pendular nystagmus with rhythmic contractions of the soft palate, resulting from disruption of the dentato-rubro-olivary pathway, or Guillain-Mollaret triangle. Oscillopsia is the most common and bothersome symptom, compared to pendular nystagmus and palatal myoclonus, which are fairly asymptomatic. T2 hyperintensity of inferior olivary nucleus (ION) typically appears within one week after brainstem injury, followed by ION hypertrophy. Given the underlying pathophysiology of ION acting as pacemaker of low-amplitude signal, treatment aimed at ION includes gabapentin and memantine. Botulinum toxin injections and surgical options have also been explored [1-2].
Method: We report the clinical and diagnostic findings of a patient with OPM secondary to brainstem hemorrhage.
Results: A 64-year-old right-handed male with a history of brainstem hemorrhage presented with binocular horizontal diplopia, oscillopsia and dysphonia one year post-hemorrhage. Neuro-ophthalmologic examination revealed varying torsional nystagmus with horizontal components. Torsion was clockwise in left gaze, counterclockwise in right gaze, and alternating between clockwise and counterclockwise in primary gaze. Palatal myoclonus synchronized with nystagmus was observed. Brain MRI demonstrated T2 hyperintensity in the left paramedian anterior medullary region [Figure 1], likely reflecting hypertrophic olivary degeneration in conjunction with gliosis and susceptibility artifact from prior hemorrhage at the level of the superior left cerebellar peduncle disrupting the Guillain-Mollaret triangle. A four-month trial of memantine provided no benefit. The patient was referred to vision rehabilitation, achieving modest improvement.
Conclusion: This case underscores the importance of recognition of OPM, characterized by pendular nystagmus, synchronized palatal myoclonus, oscillopsia, and typical MRI findings of T2 hyperintensity and hypertrophy of ION. Treatment remains challenging, with limited therapeutic options.
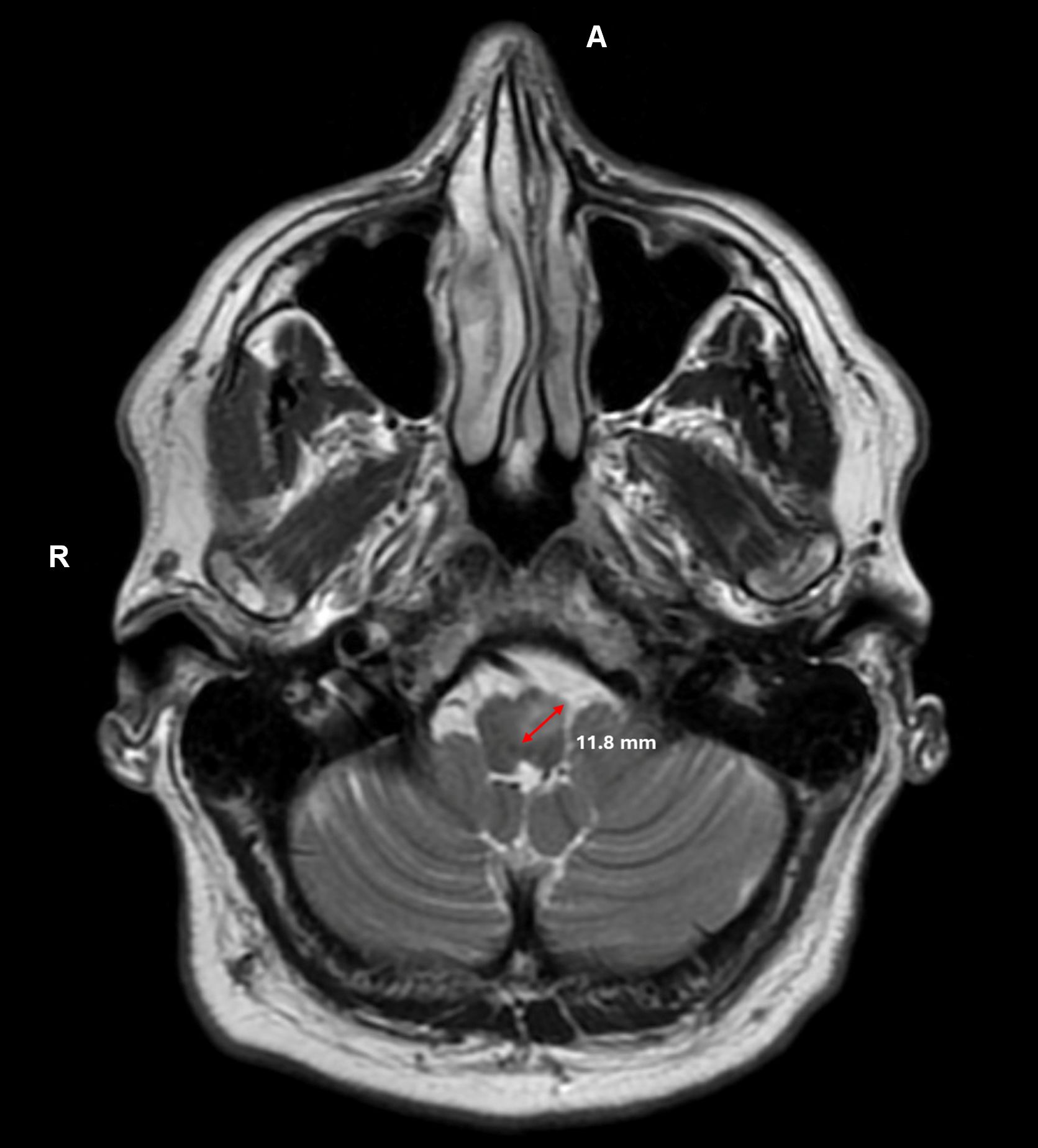
T2 hyperintensity of ION
References: 1. Borruat FX. Oculopalatal tremor: current concepts and new observations. Curr Opin Neurol. 2013;26(1):67-73. doi:10.1097/WCO.0b013e32835c60e6
2. Kim JS, Moon SY, Choi KD, Kim JH, Sharpe JA. Patterns of ocular oscillation in oculopalatal tremor: imaging correlations. Neurology. 2007;68(14):1128-1135. doi:10.1212/01.wnl.0000258665.37827.f6
To cite this abstract in AMA style:
S. Fu, U. Agarwal, T. Abu-Zahra, Z. Farzal. Oculopalatal Myoclonus Secondary to Brainstem Hemorrhage: A Case Report [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/oculopalatal-myoclonus-secondary-to-brainstem-hemorrhage-a-case-report/. Accessed April 10, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/oculopalatal-myoclonus-secondary-to-brainstem-hemorrhage-a-case-report/