Objective: This study presents the one-year outcomes of two patients who underwent unilateral deep brain stimulation (DBS) targeting the thalamic nuclei ventralis intermedius and ventralis oralis posterior (Vim/Vop) and the internal globus pallidus (GPi) for the treatment of unilateral dystonia.
Background: Unilateral dystonia, whether focal, segmental, or hemidystonia, can be treated using DBS targeting different brain regions. Simultaneous stimulation of multiple targets has been reported to provide greater benefits than stimulation of a single target1–3.
Method: A prospective assessment was conducted on an 18-year-old female with idiopathic hemidystonia of seven years’ duration causing flexion and torsion movements of the left leg and hand fingers, as well as oromandibular movements interfering with gait and speech (patient 1); and a 24-year-old male with segmental dystonia secondary to viral encephalitis suffered at the age of 2 years causing dystonic movements in the left arm, shoulder, trunk, and neck, associated with ballistic movements, significantly affecting activities of daily living (patient 2). Both patients were implanted with two DBS electrodes targeting the ipsilateral Vim/Vop and GPi as they were resistant to conservative treatment [figure1]. Microelectrode registering and macrostimulation were performed during the procedures. Both electrodes were placed through a single burr hole. Clinical outcomes were evaluated preoperatively and one year after initiating simultaneous stimulation of both nuclei using the Burke-Fahn-Marsden Dystonia Rating Scale (BFMDRS), which comprises a movement subscale (BFMMS) and a disability subscale (BFMDS).
Results: The minimal clinically important difference (MCID) for BFMMS has been defined as an improvement >16.6%4. Concerning baseline BFMMS values, patients 1 and 2 exhibited an improvement of threefold and fivefold the MCID, respectively, at the 12-month follow-up. The MCID for the BFMDS has been established at 0.5 points. With respect to the baseline BFMDS values, patients 1 and 2 demonstrated an improvement of fourfold and sixfold the MCID at the 12-month follow-up. None of the patients experienced complications related to the surgical procedures.
Conclusion: Both patients showed significant improvement in their dystonia. Simultaneous stimulation of Vim/Vop and GPi may be equally or more effective than stimulation of a single target.
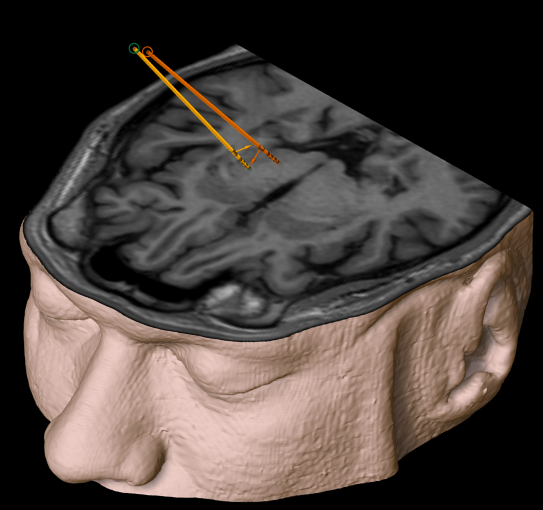
figure1
References: 1. Slotty PJ, Poologaindran A, Honey CR. A prospective, randomized, blinded assessment of multitarget thalamic and pallidal deep brain stimulation in a case of hemidystonia. Clin Neurol Neurosurg. 2015;138:16-19. doi:10.1016/j.clineuro.2015.07.012
2. Chang KW, Kim MJ, Park SH e investigacion/MER D distonia AAD-2022-W-SNSILFPC in D pd., Chang WS, Jung HH, Chang JW. Dual Pallidal and Thalamic Deep Brain Stimulatifor Complex Ipsilateral Dystonia. Yonsei Med J. 2022;63(2):166-172. doi:10.3349/ymj.2022.63.2.166
3. Goulenko V, Cruz PL da C, Filho PN. Unilateral thalamic and pallidal deep brain stimulation for idiopathic hemidystonia: Results of individual and combined stimulations. Case report. Neurosurg Focus. 2017;43(1):1-5. doi:10.3171/2017.4.FOCUS17134
4. Pintér D, Janszky J, Kovács N. Minimal Clinically Important Differences for Burke-Fahn-Marsden Dystonia Rating Scale and 36-Item Short-Form Health Survey. Mov Disord. 2020;35(7):1218-1223. doi:10.1002/mds.28057
To cite this abstract in AMA style:
J. Altamirano, K. Salinas-Barboza, A. Armas-Salazar. One-Year Outcomes of Multitarget Thalamic and Pallidal Deep Brain Stimulation in Unilateral Dystonia [abstract]. Mov Disord. 2024; 39 (suppl 1). https://www.mdsabstracts.org/abstract/one-year-outcomes-of-multitarget-thalamic-and-pallidal-deep-brain-stimulation-in-unilateral-dystonia/. Accessed August 5, 2026.« Back to 2024 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/one-year-outcomes-of-multitarget-thalamic-and-pallidal-deep-brain-stimulation-in-unilateral-dystonia/