Category: Rare Genetic and Metabolic Diseases
Objective: Our aim was to assess the efficacy and safety of trientine tetrahydrochloride (TETA4HCL) in a cohort of neurological Wilson’s disease (WD) patients transitioned from D-penicillamine (DP) to TETA4HCL on a 1:0.5 (mg:mg) total daily dose basis.
Background: TETA4HCL serves as an alternative copper chelating agent for WD patients intolerant to D-penicillamine (DP). However, there are currently no established guidelines for the dose transition between DP and TETA4HCL, nor available data on outcomes.
Method: Neurological patients treated with DP for at least six months and subsequently switched to TETA4HCL were prospectively reported in the French WD registry. Unified Wilson Disease Scores (UWDRS), Clinical Global Impression (CGI), hepatic (liver enzymes, APRI score, Fibroscan), and copper parameters (exchangeable copper (ExCu) which corresponds to the direct dosage of non-ceruloplasmin bound copper, and 24h-urinary copper excretion (UCE)) were assessed at baseline and at two years of follow-up. Doses of TETA4HCL and outcomes were documented.
Results: Twenty-four patients, with a median age of 41.3 years (IQR: 34.3-49.5), who had been treated with 900 mg/day of DP for a median of 14 years (IQR: 8.5-27.8), were switched to TETA4HCL (450 mg/day) due to DP-related side effects.
After two years (see table), there was no change in the CGI improvement score, and UWDRS and ExCu values remained stable. However, despite a 25% increase in the dose of TETA4HCL and improved adherence to treatment, transaminase levels increased over time (ALT>AST). TETA4HCL was discontinued in one patient due to liver failure. Tolerance was very good.
Conclusion: The transition from DP to TETA4HCL demonstrated neurological and ExCu stability, improved adherence, and a favorable safety profile. However, the subsequent increase of liver enzymes raises questions about the optimal doses of TETA4HCL required as oral maintenance therapy to prevent progressive copper overload. Switching from DP to TETA4HCL should be done with a minimal ratio of 0.8 with close follow-up of clinical symptoms, liver tests and copper metabolism (ExCu and UCE).
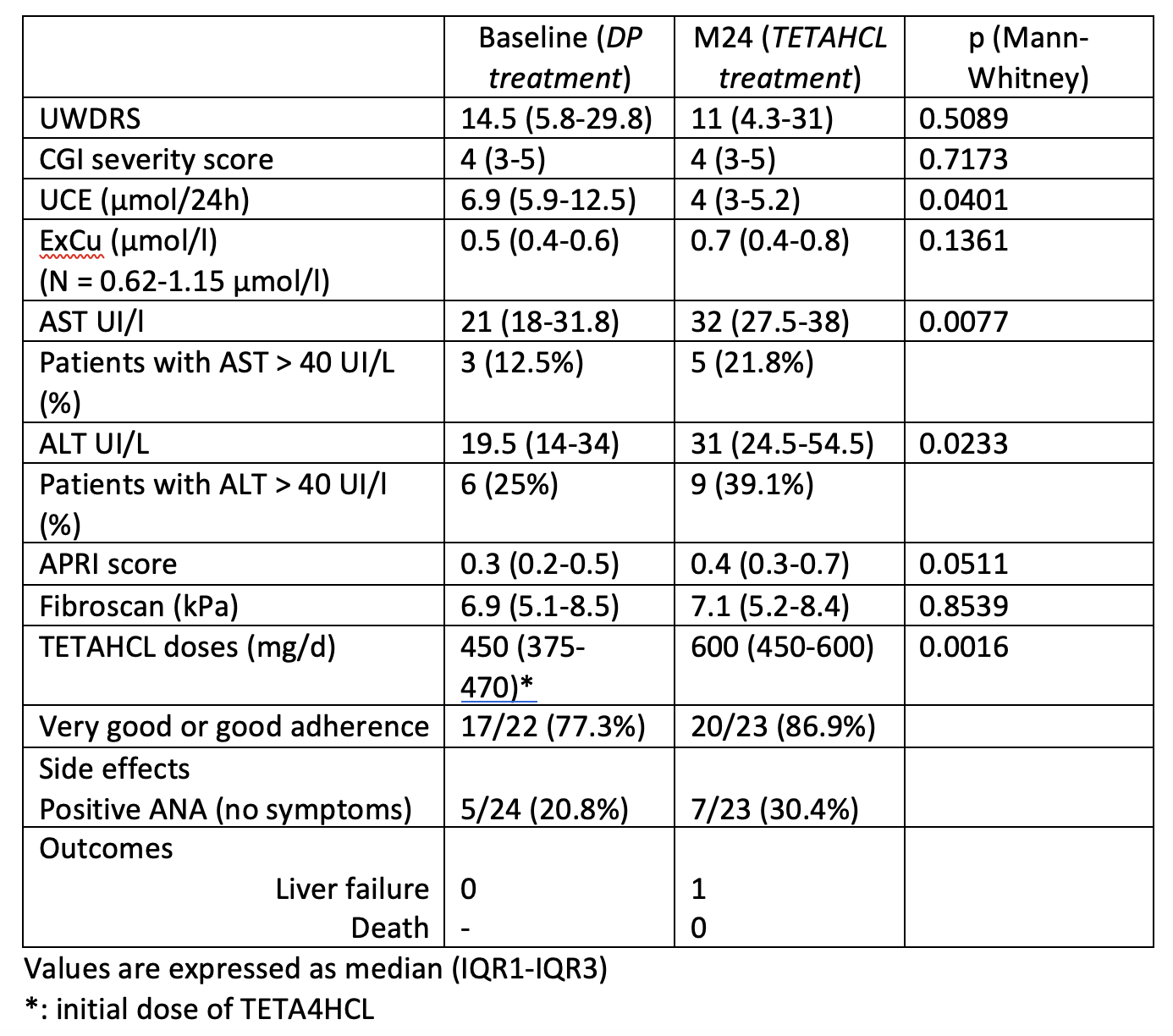
Table
To cite this abstract in AMA style:
A. Poujois, MA. Obadia, N. Oussedik-Djebrani, E. Couchonnal-Bedoya, D. Debray. Real-life experience of switching from D-penicillamine to trientine tetrahydrochloride – a nationwide registry study [abstract]. Mov Disord. 2024; 39 (suppl 1). https://www.mdsabstracts.org/abstract/real-life-experience-of-switching-from-d-penicillamine-to-trientine-tetrahydrochloride-a-nationwide-registry-study/. Accessed August 6, 2026.« Back to 2024 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/real-life-experience-of-switching-from-d-penicillamine-to-trientine-tetrahydrochloride-a-nationwide-registry-study/