Category: Huntington's Disease
Objective: To estimate risk of Huntington’s disease (HD) over time in patients with reduced penetrance (RP) alleles (36-39 CAG repeats) overall, by individual repeat length, by sex, and compared to patients in the full penetrance (FP) range (40+ repeats).
Background: HD is a fatal autosomal dominant neurodegenerative disorder, caused by a CAG repeat expansion in the huntingtin gene. For those with 40+ repeats, for whom penetrance is 100%, several estimates of disease onset have been published. Less is known about the prognosis for RP patients.
Method: Prospective observational data from pre-manifest HD gene expansion carriers who participated in the PREDICT-HD and Enroll-HD studies were analyzed. Kaplan-Meier (KM) curves that account for left-truncation were fit to estimate age of manifest HD diagnosis, defined as a diagnostic confidence level (DCL) of 4 on the unified Huntington’s disease rating scale. Those who remained diagnosis-free were censored at their last known DCL. Log-rank tests were performed at a 5% significance level.
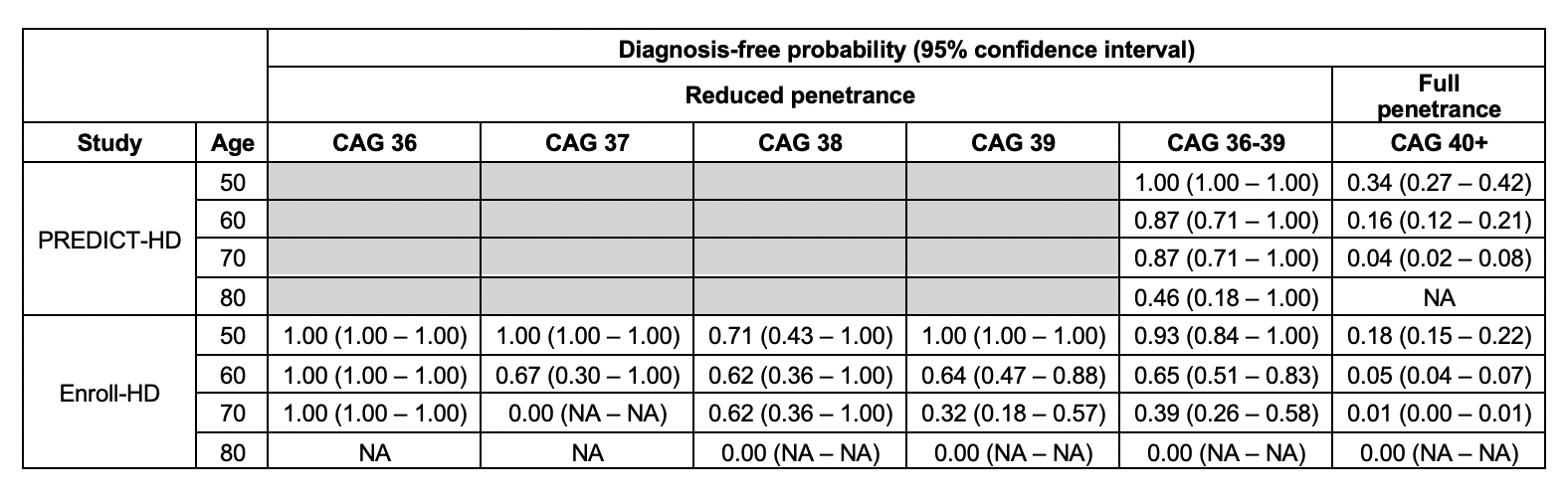
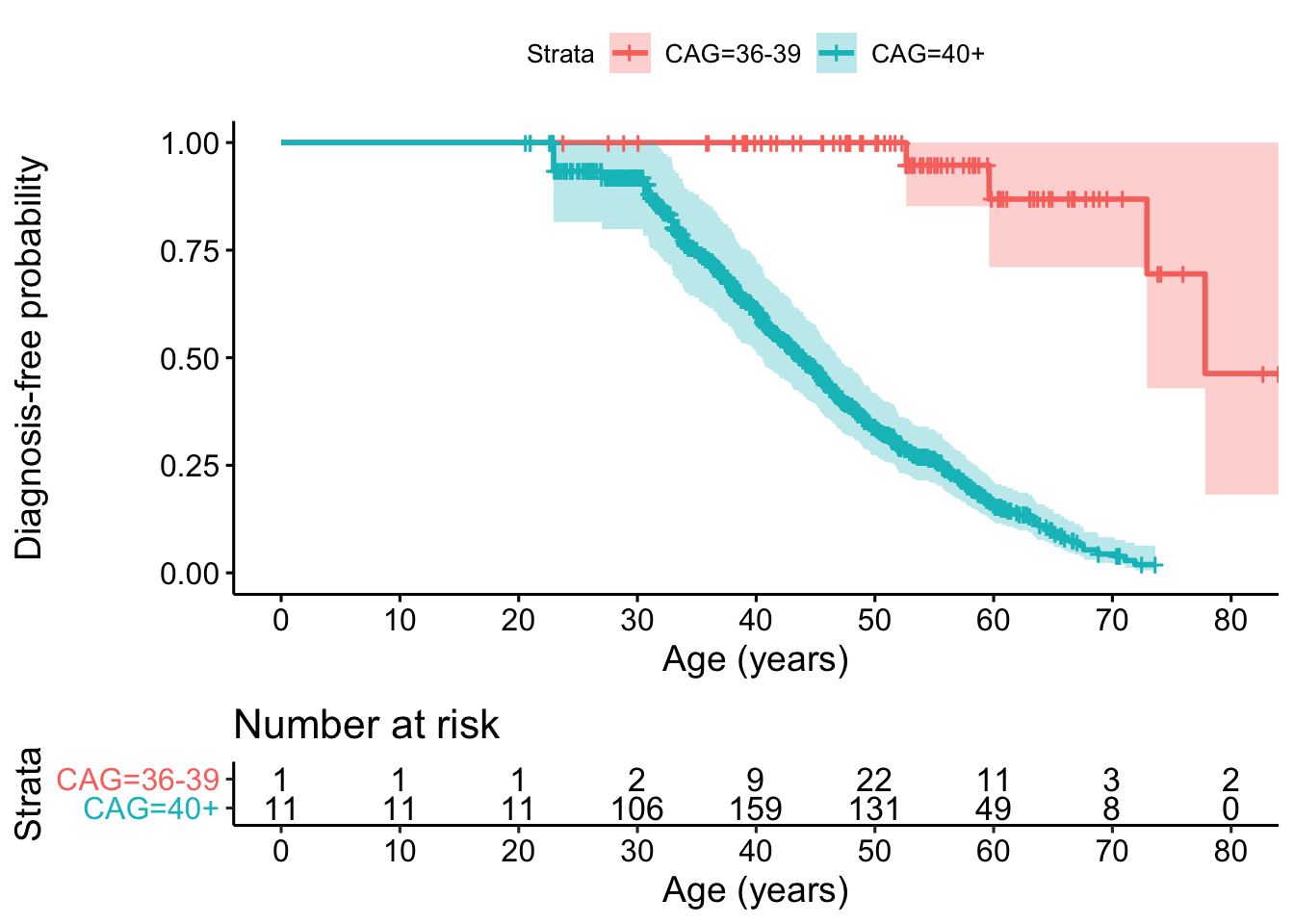
Results: For PREDICT-HD, 87 RP and 914 FP patients were analyzed. Among them, 4 RP patients (all with 39 repeats) and 240 FP patients eventually reached manifest HD. Median follow up time for censored patients was 4.1 years. Diagnosis-free probabilities for RP and FP patients at various ages are presented in [table1]. Diagnosis was significantly delayed in RP vs. FP patients (p<0.001) [figure1].
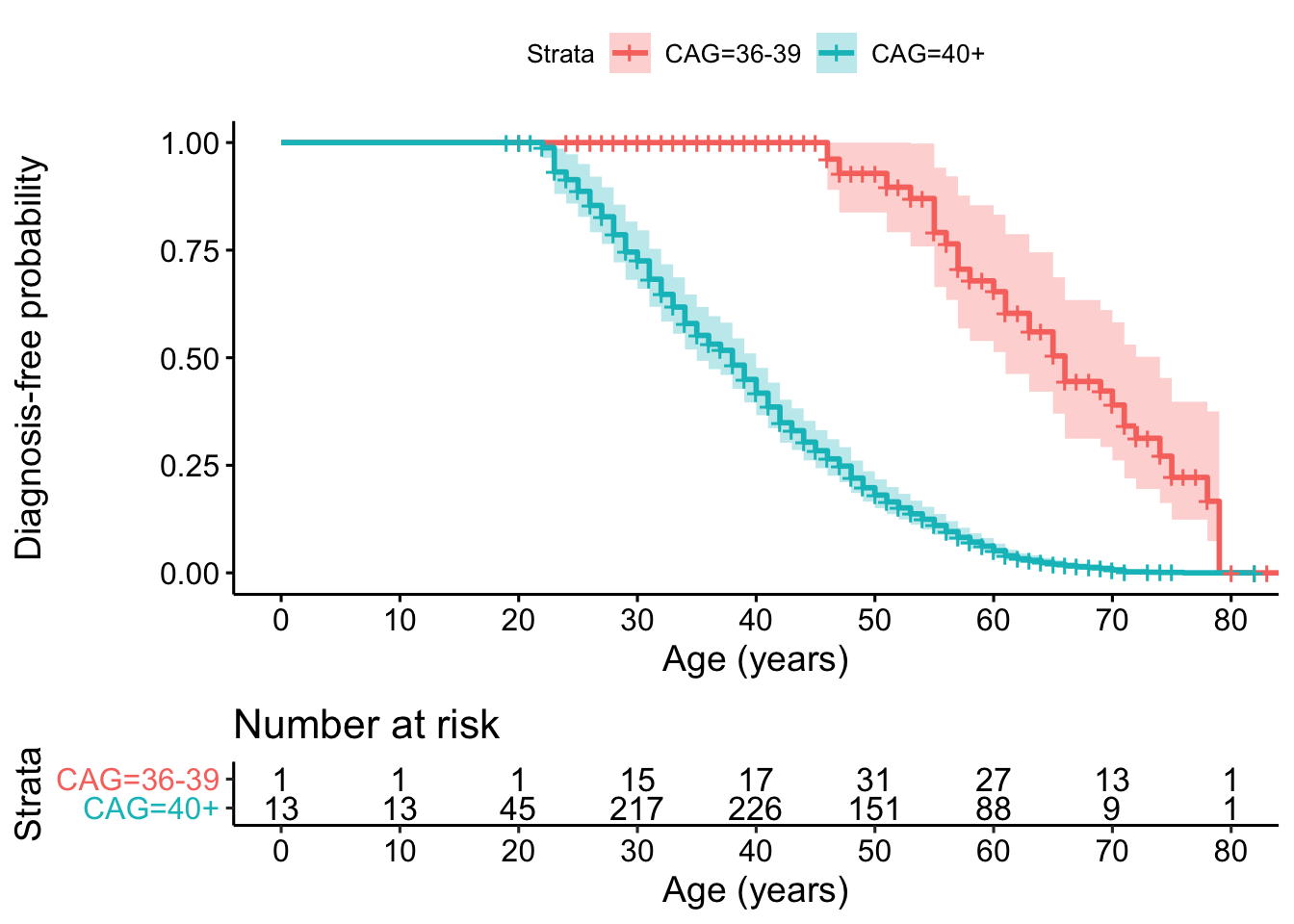
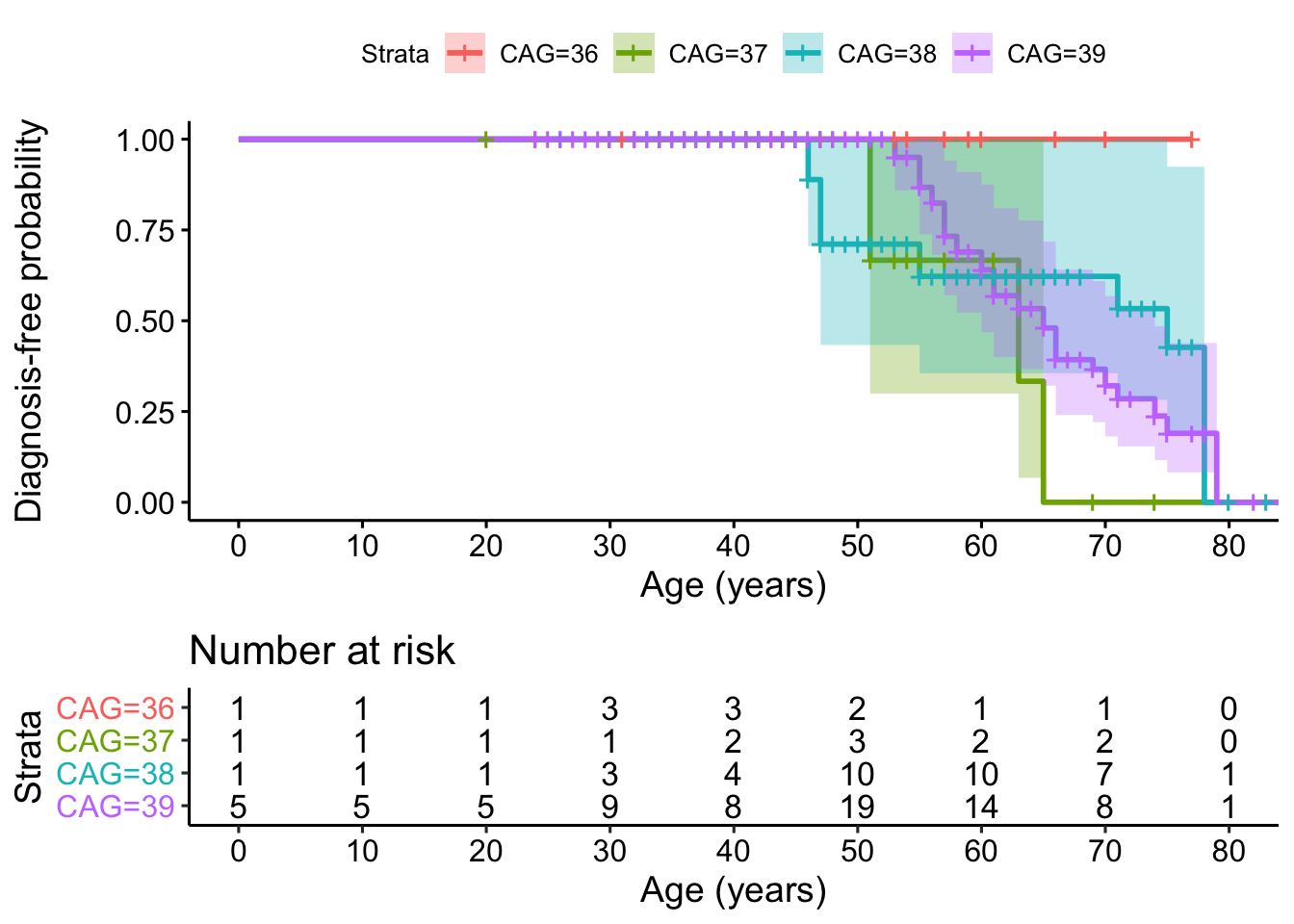
For Enroll-HD, among 403 RP patients, 35 eventually phenoconverted, 23 of whom had 39 repeats and none of whom had 36 repeats. Compared to FP patients (N = 3,088 with 572 phenoconverters), diagnosis was significantly delayed in RP patients (p<0.001) [figure2]. Diagnosis-free probabilities for RP and FP patients as well as individual repeat lengths in the RP range are presented in [table1]. Age of diagnosis in RP patients did not differ by individual CAG repeat length (p=0.7) [figure3] or sex (p=0.8).
Conclusion: Data from two studies show significant delay in HD onset in patients with 36-39 CAG repeats vs. 40+. We estimated age-specific probabilities of remaining diagnosis-free by individual repeat length in the RP range and found no significant difference. One limitation may be heterogeneity in DCL scores due to difficulty in interpreting neurological examinations at older ages. Future work is needed to 1) combine data sources to improve precision and 2) incorporate competing risks such as death.
To cite this abstract in AMA style:
E. Mcdonnell, Y. Wang, K. Marder. Risk and timing of manifest Huntington’s disease in patients with reduced penetrance alleles [abstract]. Mov Disord. 2021; 36 (suppl 1). https://www.mdsabstracts.org/abstract/risk-and-timing-of-manifest-huntingtons-disease-in-patients-with-reduced-penetrance-alleles/. Accessed July 4, 2026.« Back to MDS Virtual Congress 2021
MDS Abstracts - https://www.mdsabstracts.org/abstract/risk-and-timing-of-manifest-huntingtons-disease-in-patients-with-reduced-penetrance-alleles/