Category: Ataxia
Objective: To report and extend the clinical and radiological features of Progressive Ataxia and Palatal Tremors (PAPT) syndrome.
Background: Hypertrophic degeneration of olivary nucleus is a consequence of damage to tracts in the Guillain Mollaret triangle. It presents as palatal tremors (formerly palatal myoclonus) involving soft palate, pharynx, uvula, larynx with oculopalatal tremors or without ocular involvement. Midline form is associated with bilateral olivary hypertrophy.
Method: A 34-year-old female with history of primary infertility and no family history presented with history of progressive gait imbalance, titubation and tremulousness of voice developing over 1 year. She also had urinary urge incontinence. On examination, she had normal cognition. Asynchronous nystagmoid eye movements were noted with fast component to the right on looking rightward and upwards along with hypermetric saccades and saccadic pursuit. She had 2-3 Hz palatal tremors with no audible clicks; normal palatal movements and gag reflex were present. Motor and sensory examination were normal. Cerebellar examination unveiled prominent gait ataxia alone. Finger-nose test and knee-heel test were normal. Additionally, titubation was noted. Extra pyramidal examination was normal.
Results: Routine blood investigations including serum autoimmune panel, anti-TTG and thyroid profile were normal. Nerve conduction studies and autonomic function tests were normal. Uroflometric studies were also normal. MRI brain showed bilateral hypertrophied inferior olivary nuclei (Figure 1). Whole exome sequencing revealed no pathogenic variants. CSF studies including autoimmune panel, oligoclonal bands and PCR for T. whippeli were negative. PET CT brain was suggestive of mild hypermetabolism along bilateral basal ganglia. The patient was initiated on oral Prednisolone (1mg/kg) for presumptive autoimmune encephalitis along with slowly titrated Propranolol (Dose 80mg/day) and gait/balance rehabilitation. The patient reported no improvement at six months of follow up, and steroids were tapered off.
Conclusion: We report a patient with sporadic PAPT syndrome with likely midline form of asynchronous oculopalatal tremors and gait ataxia with bilateral olivary hypertrophy without a structural lesion.
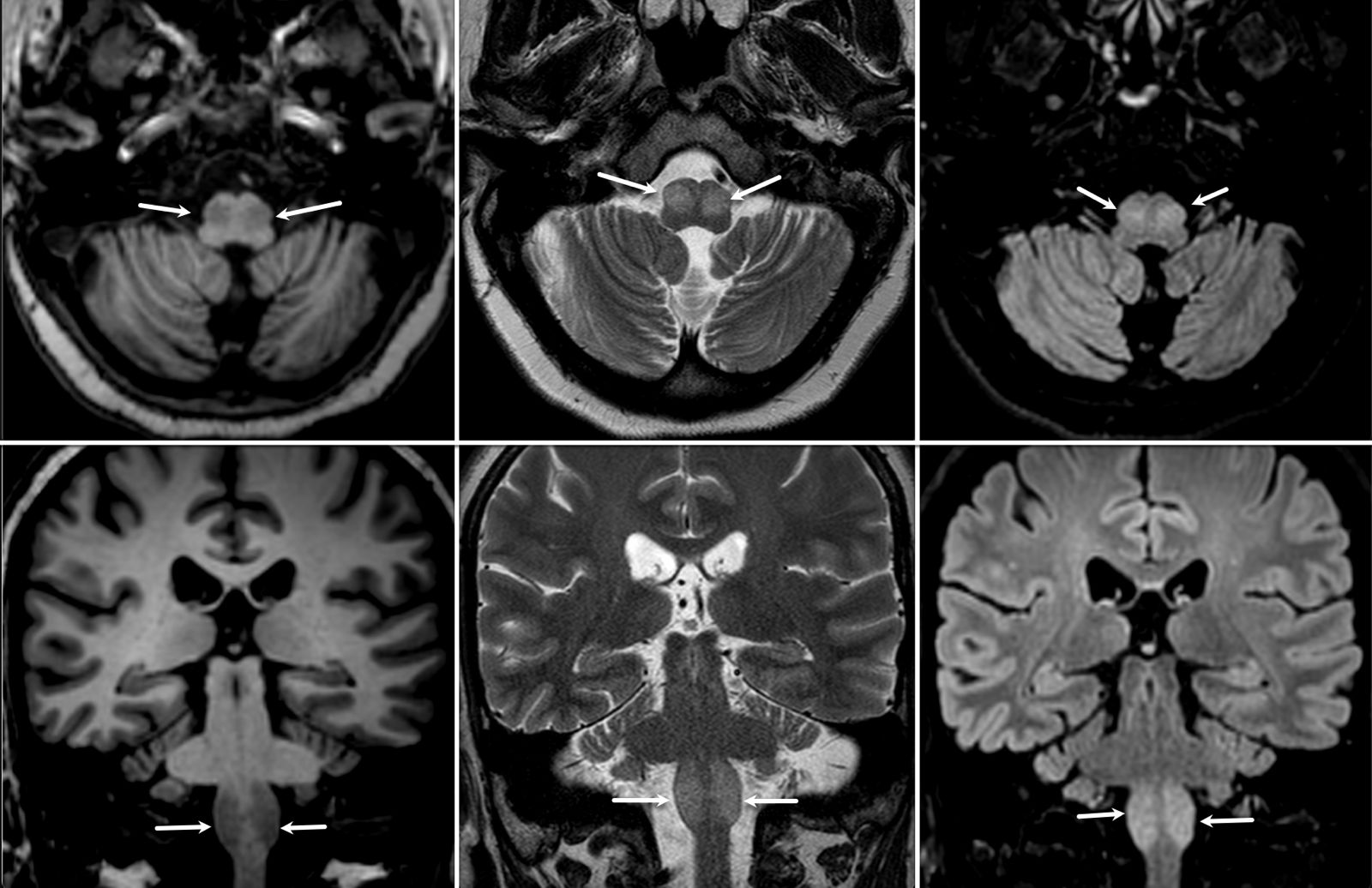
Bilateral hypertrophied inferior olivary nuclei
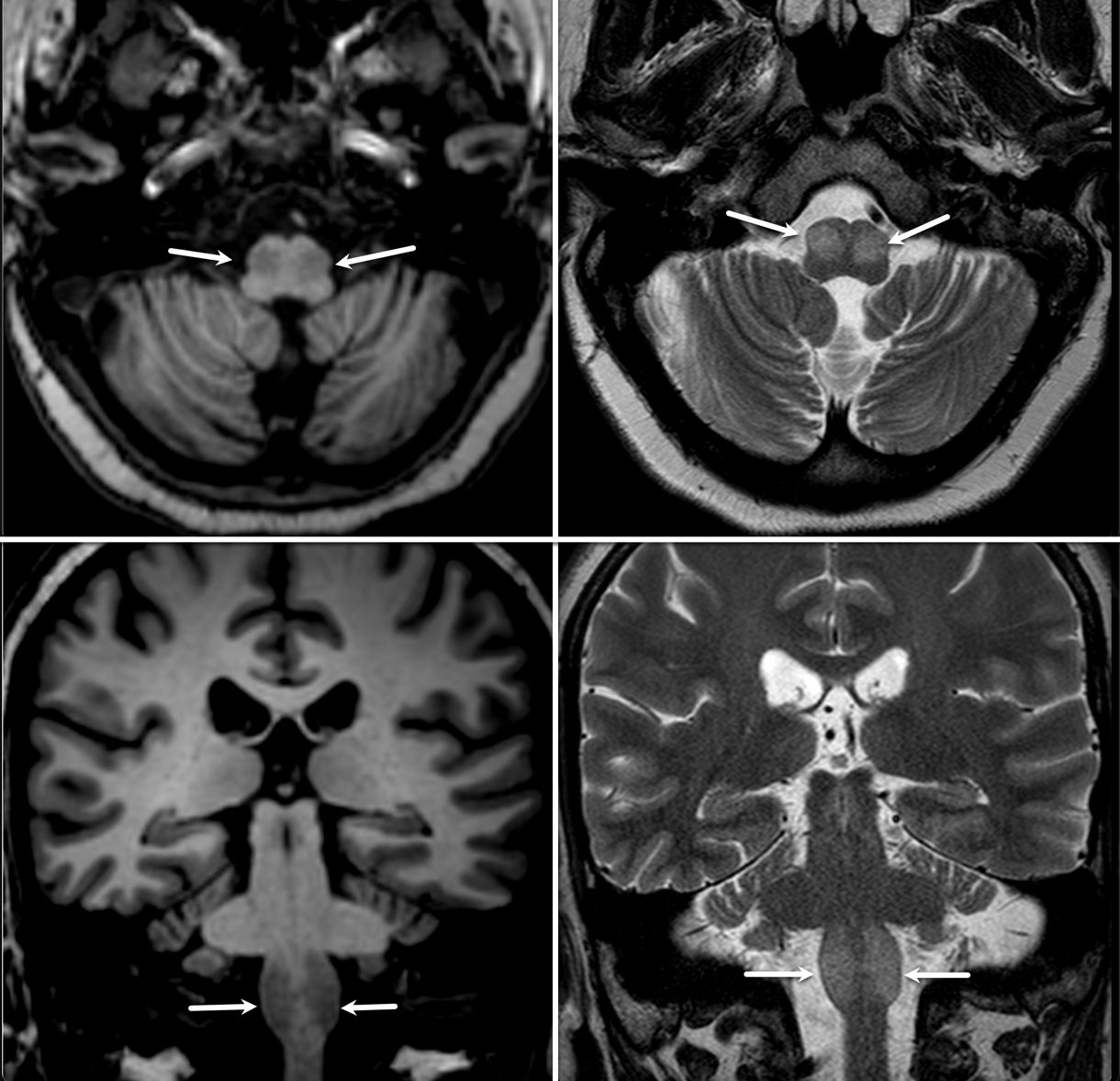
Bilateral hypertrophied inferior olivary nuclei
To cite this abstract in AMA style:
P. Saroja Bylappa, D. Garg, A. Agarwal, A. Garg, A. Srivastava. Syndrome of Progressive Ataxia with Palatal Tremors (PAPT) with Hypertrophied Bilateral Inferior Olives in a young Indian Female [abstract]. Mov Disord. 2024; 39 (suppl 1). https://www.mdsabstracts.org/abstract/syndrome-of-progressive-ataxia-with-palatal-tremors-papt-with-hypertrophied-bilateral-inferior-olives-in-a-young-indian-female/. Accessed August 8, 2026.« Back to 2024 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/syndrome-of-progressive-ataxia-with-palatal-tremors-papt-with-hypertrophied-bilateral-inferior-olives-in-a-young-indian-female/