Category: Parkinson's Disease: Surgical Therapy
Objective: We describe the changes occurring in LFP dynamics in a Parkinson’s disease (PD) patient recovering from post-implant unilateral edema after deep brain stimulation (DBS) implant.
Background: DBS of the globus pallidus internus (GPi) is an established therapy for PD. Increased beta-band activity, measurable via LFP recordings, correlates with symptom severity. However, whether hypersynchronized beta activity in PD originates from motor cortex or basal ganglia remains debated.
Method: A man in his fifties underwent bilateral GPi-DBS (Medtronic PerceptPC; Sensight B33005 leads) for PD. After surgery, LFP power spectra were recorded from all possible bipolar configurations per side via BrainSense signal test. Additionally, chronic sensing of the most prominent peak beta frequency (ten-minutes average of the 5Hz window around the selected peak) was activated. Postoperative CT showed frontal pneumocephalus without major bleeding or edema, and the patient had no focal deficits. Two days later, the subject developed left hemiparesis. Urgent CT revealed massive peri-lead edema and pneumocephalus, eventually requiring decompression. Over one-month, chronic beta-peak sensing and repeated neuroimaging/LFP power spectra assessments were performed.
Results: Initial LFP recordings showed a typical stun-effect pattern bilaterally (Figure1). As massive right-hemisphere edema (extending from frontal cortex to GPi) developed, beta activity remained suppressed, while the left side gradually regained over time. Beta suppression in the right GPi persisted despite radiological resolution of pallidal edema (Figure2). However, as right motor cortex edema resolved, beta hyperactivity re-emerged, coinciding with hemiparesis resolution. A non-significant inverse correlation between edema volume and right GPi mean beta power was observed (Figure3). Alpha and gamma activity showed the same dynamics in both nuclei.
Conclusion: This case represents an incidental lesional model of cortico-pallidal disconnection in PD. LFPs recordings showed persistent band-specific beta suppression in the right GPi despite nuclear recovery, lasting until motor cortex edema resolved, whereas the unaffected hemisphere exhibited a normal stun effect. These findings suggest that beta hypersynchronization in PD primarily depends on motor cortex integrity rather than GPi function.
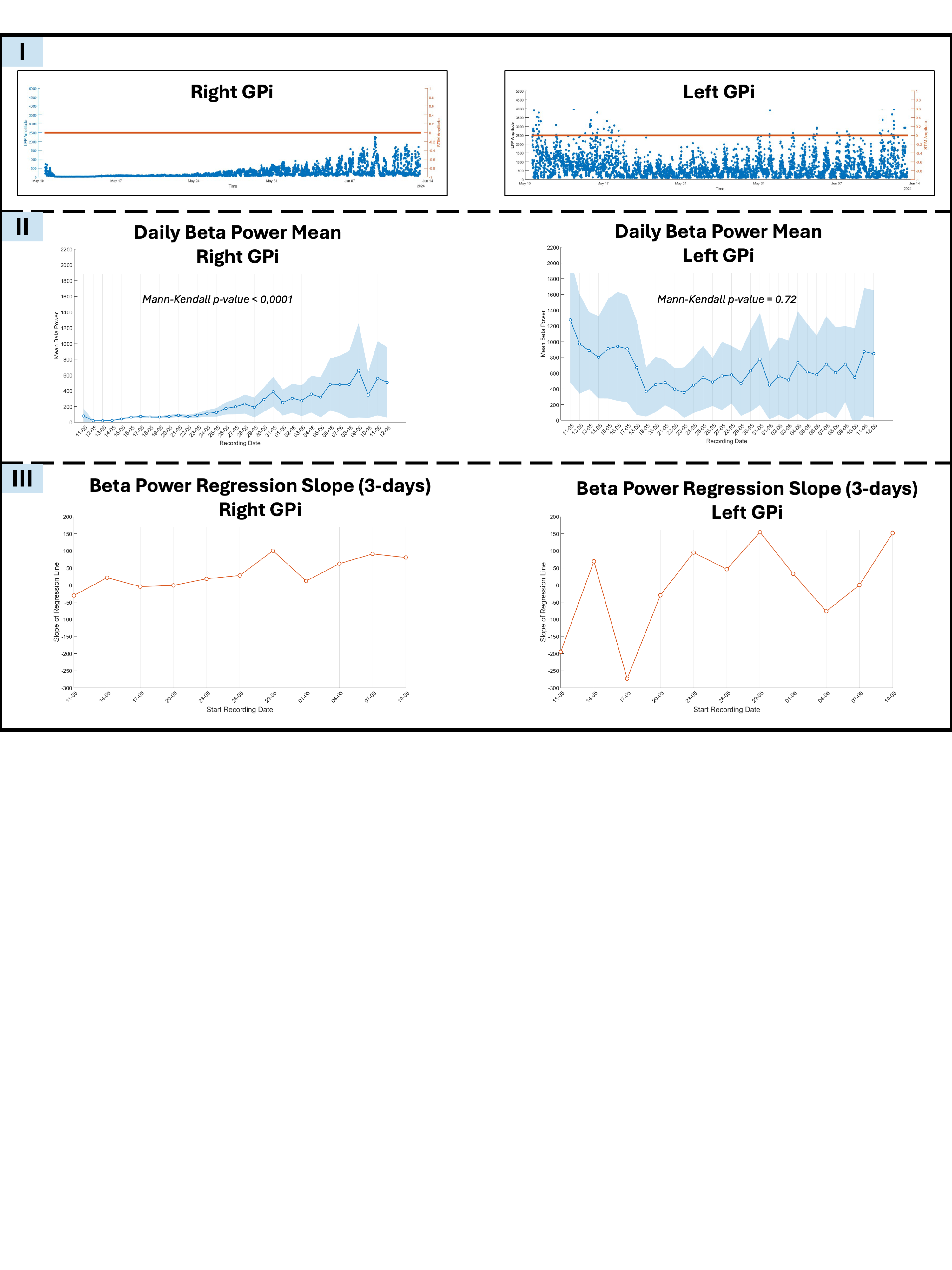
Persistent beta suppression in rightGPi
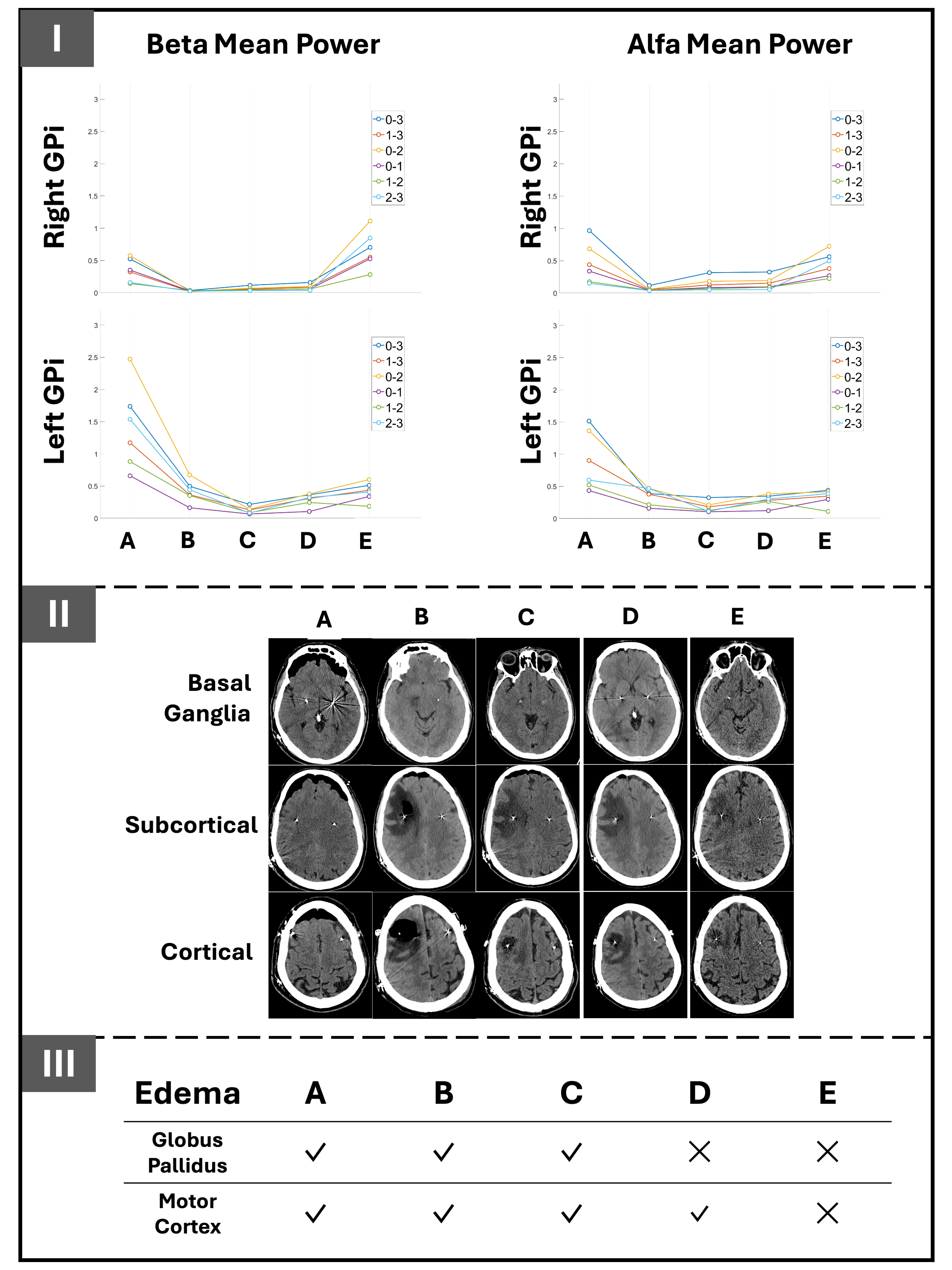
LFP dynamics and brain edema evolution
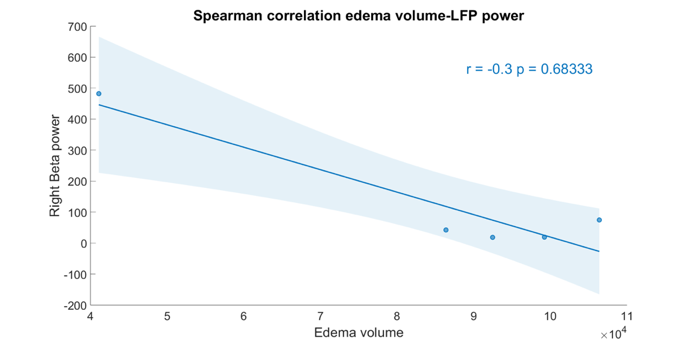
RightGPi beta power and edema volume correlation
References: Tinkhauser, Gerd et al. “Beta burst coupling across the motor circuit in Parkinson’s disease.” Neurobiology of disease vol. 117 (2018): 217-225. doi:10.1016/j.nbd.2018.06.007
To cite this abstract in AMA style:
L. Rigon, V. D'Onofrio, LL. Grassi, A. Antonini, A. Guerra. Where does excessive beta in Parkinson’s disease originate? Insights from a case of unilateral cortico-pallidal disconnection [abstract]. Mov Disord. 2025; 40 (suppl 1). https://www.mdsabstracts.org/abstract/where-does-excessive-beta-in-parkinsons-disease-originate-insights-from-a-case-of-unilateral-cortico-pallidal-disconnection/. Accessed April 8, 2026.« Back to 2025 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/where-does-excessive-beta-in-parkinsons-disease-originate-insights-from-a-case-of-unilateral-cortico-pallidal-disconnection/