Category: Parkinson's Disease: Neurophysiology
Objective: To determine the impact of liver fibrosis on motor symptoms in Parkinson’s disease
Background: Parkinson’s disease motor symptoms can vary with systemic illnesses [1,2]. A subset of individuals with end-stage liver disease develop parkinsonism [3], suggesting that the pathways dysregulated in Parkinson’s disease are vulnerable to disturbances of the brain-liver axis. However, the impact of hepatic dysfunction on the motor manifestations of Parkinson’s disease remains unknown.
Method: We conducted a retrospective cohort study using data from the Parkinson’s Progression Markers Initiative collected between 2010 and 2023. Liver disease was defined using the validated Fibrosis-4 (FIB-4) score. Our primary outcome was the association of the baseline FIB-4 score with MDS-Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) part 3 score. FIB-4 scores were also compared with rigidity, bradykinesia, tremor and gait subsections of the MDS-UPDRS part 3. Additional outcome measures were the MDS-UPDRS part 2 score and Hoehn and Yahr stages. We used linear regression models to assess the relationship between liver fibrosis and motor scores at baseline. Models were adjusted for demographics, comorbidities, alcohol use, and baseline cognitive, psychiatric, and autonomic function.
Results: We included 537 participants (mean age 61.8, 39.9% women). There was a significant association between liver fibrosis and baseline MDS-UPDRS part 3 scores (β=2.8, p=0.0015). Elevated FIB-4 scores were associated with increased rigidity (β=0.86 p=5.7×10-4) and bradykinesia (β=1.2 p=0.020). There was no significant relationship with baseline MDS-UPDRS part 2 scores or Hoehn and Yahr stages.
Conclusion: In Parkinson’s disease, comorbid liver fibrosis was associated with more severe motor deficits early in the disease course. FIB-4 scores were linked with increased rigidity, bradykinesia, suggesting that circuits controlling these functions may be especially vulnerable to liver dysfunction. Further work is required determine whether liver fibrosis impacts motor performance through global mechanisms or specifically nigrostriatal pathways and how liver fibrosis impacts disease progression. Counseling patients to preserve liver health through the avoidance of excess alcohol use and dietary modifications may be reasonable.
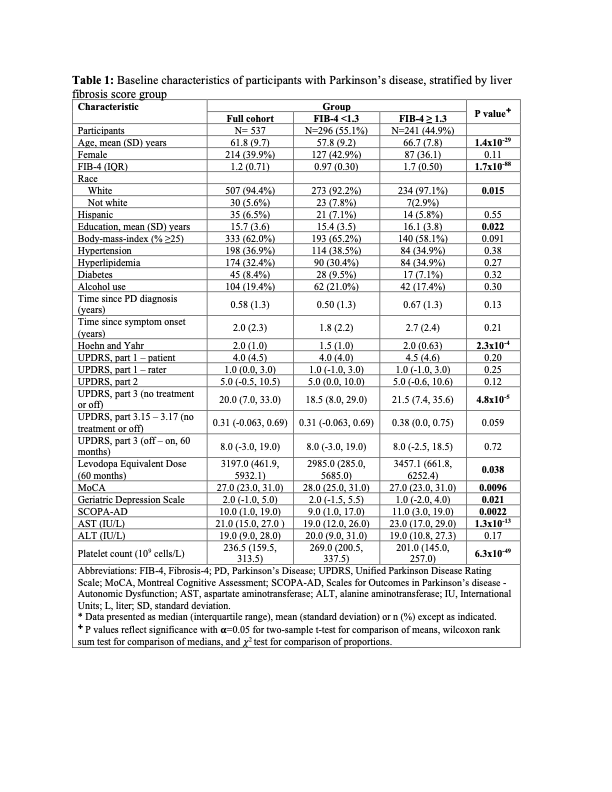
Table 1
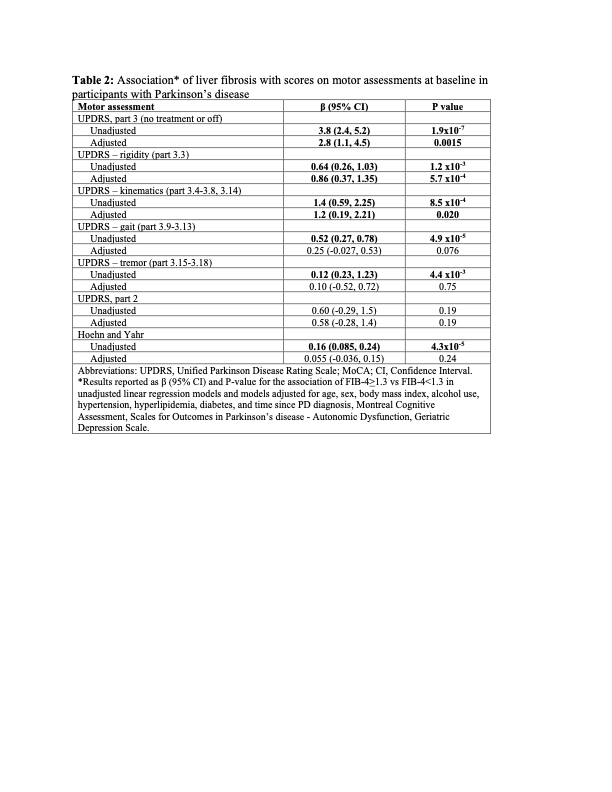
Table 2
References: 1. Potashkin, J. et al. Understanding the links between cardiovascular disease and Parkinson’s disease. Mov. Disord. Off. J. Mov. Disord. Soc. 35, 55–74 (2020).
2. Cheong, J. L. Y., de Pablo-Fernandez, E., Foltynie, T. & Noyce, A. J. The Association Between Type 2 Diabetes Mellitus and Parkinson’s Disease. J. Park. Dis. 10, 775–789.
3. Apetauerova, D. et al. A Prospective Study of the Prevalence of Parkinsonism in Patients With Liver Cirrhosis. Hepatol. Commun. 5, 323–333 (2021).
To cite this abstract in AMA style:
A. Zolin, H. Ooi, H. Sarva. Association of Liver Fibrosis with Motor Deficits in Parkinson’s Disease [abstract]. Mov Disord. 2024; 39 (suppl 1). https://www.mdsabstracts.org/abstract/association-of-liver-fibrosis-with-motor-deficits-in-parkinsons-disease/. Accessed July 4, 2026.« Back to 2024 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/association-of-liver-fibrosis-with-motor-deficits-in-parkinsons-disease/