Category: Choreas (Non-Huntington's Disease)
Objective: To report a case of chorea hyperglycemia basal ganglia syndrome (CHBG) with normal glucose.
Background: Elderly persons with CHBG usually have high glucose (average 414 mg/dL) on presentation1. CT brain often shows a hyperattenuation in the basal ganglia, and MRI brain usually shows a T1 hyperintensity in the putamen. The chorea often improves with glycemic control. About 20% of cases have a recurrence of the chorea, even after MRI shows resolution.1
Method: NA
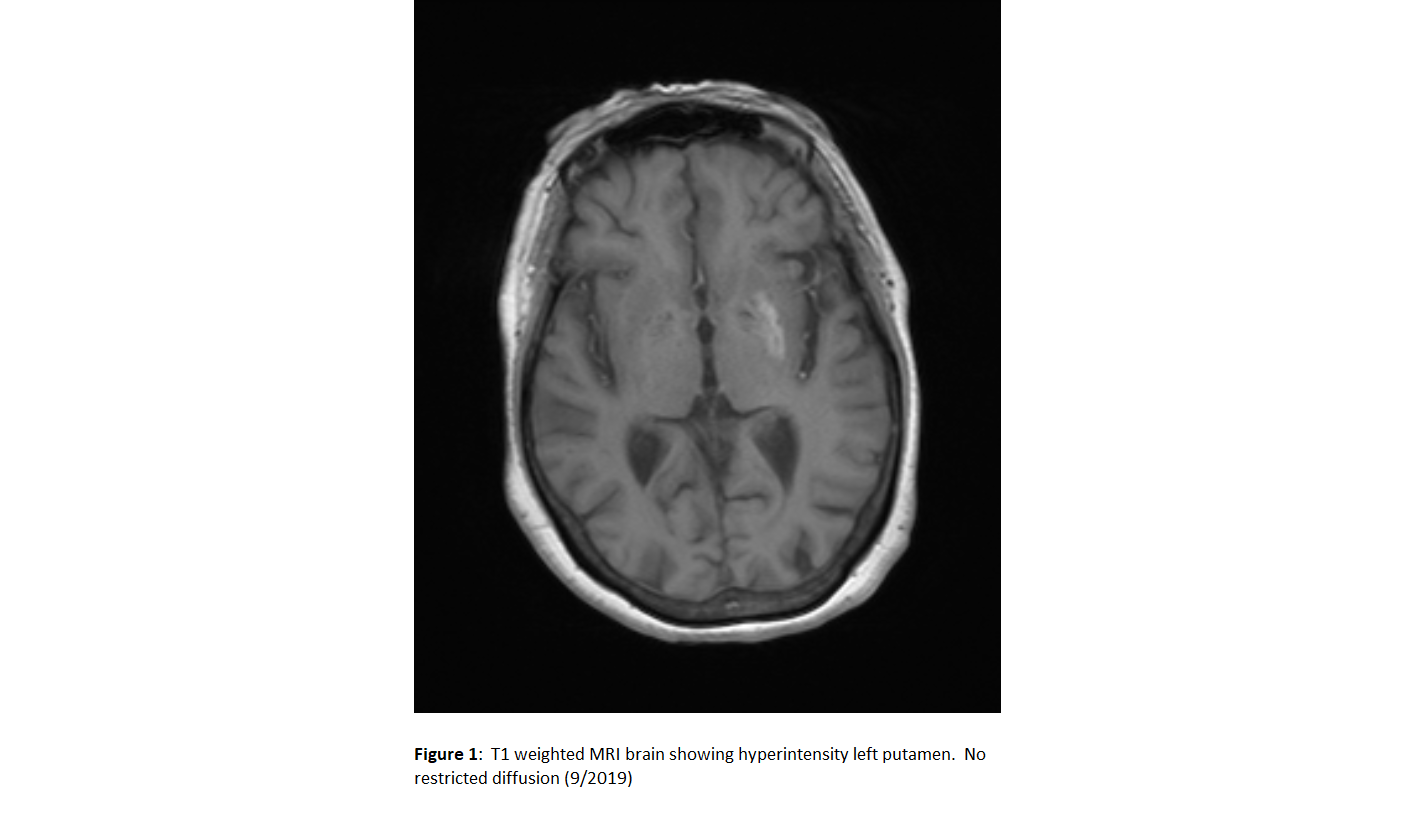
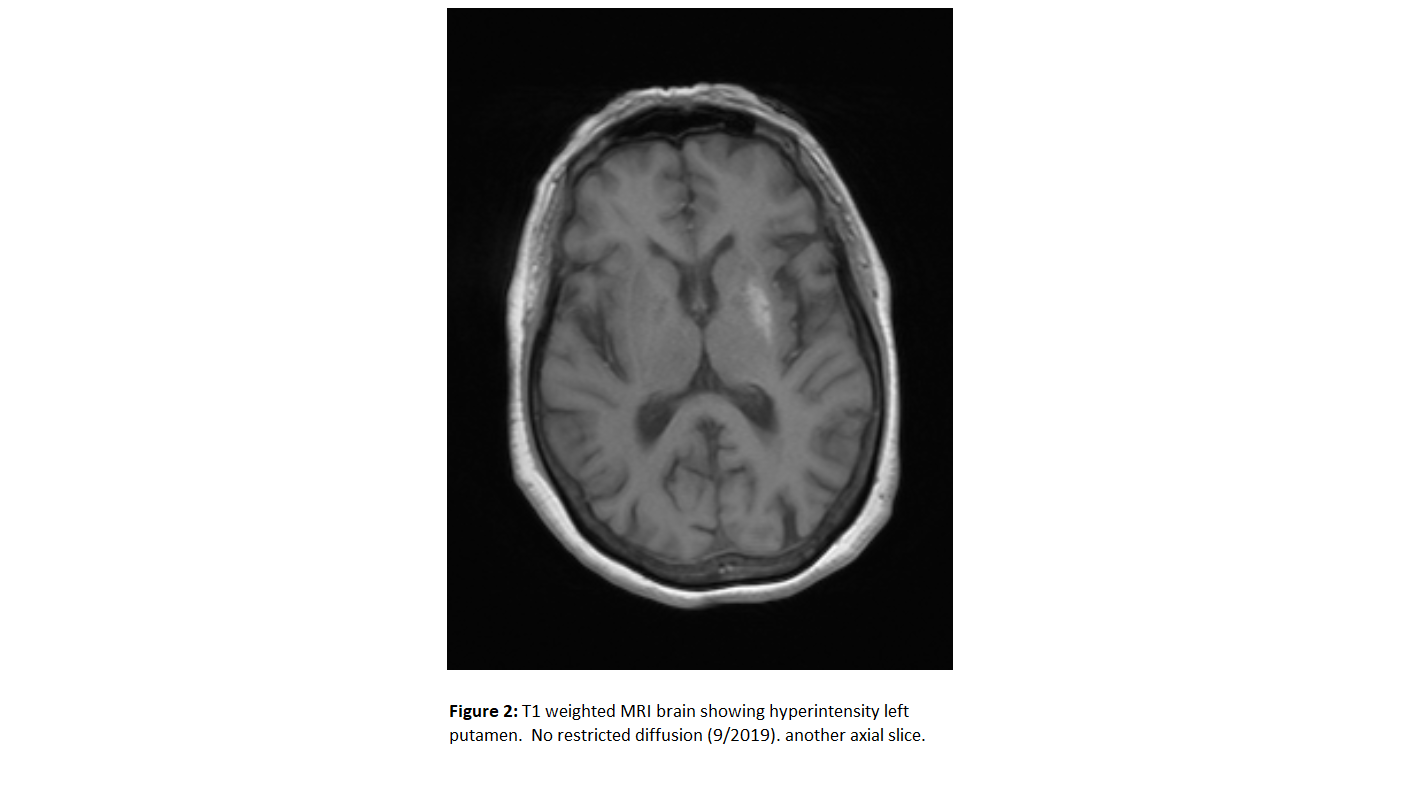
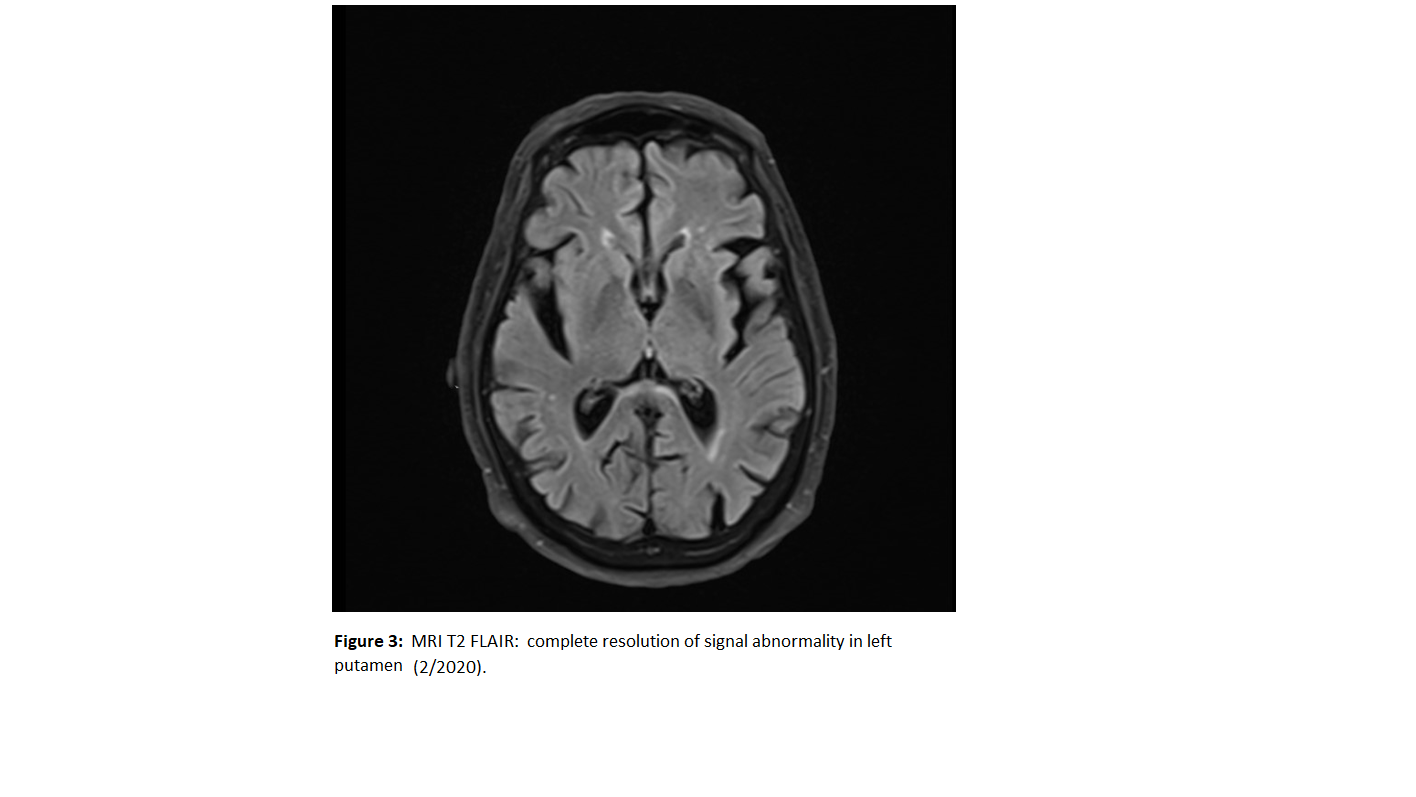
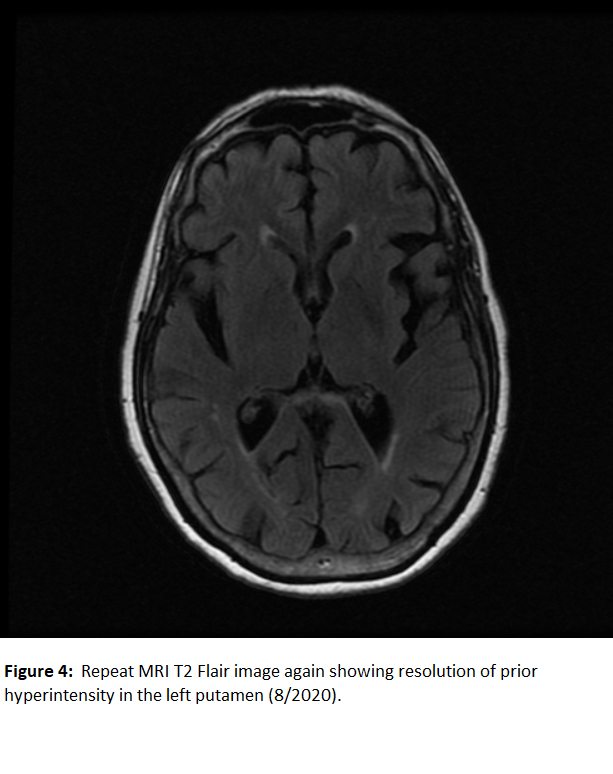
Results: A 76-year-old Hispanic female with type 2 diabetes and rheumatoid arthritis (on prednisone) first presented to the hospital with weakness of the right side. No chorea was found then. Serum glucose was 720 mg/dL. Hba1c was 12.9%. MRI Brain showed chronic white matter disease but nothing acute. Symptoms resolved and she was discharged as a TIA. Three weeks later at home, she developed a right hemichorea, but did not seek medical attention. Two weeks later, she went to the hospital, and was found to have a chorea of the right leg and right arm, sparing face and trunk. Repeat MRI Brain showed increased T1 signal of the left putamen not seen on the prior MRI (Figs 1,2). DWI was negative for ischemia. Admission serum glucose was 92 mg/dL. Urine ketones none. AST, ALT, and TSH were all normal. CSF: WBC 3, protein 52, glucose 113 (normal < 70). Oligoclonal bands none. Sed rate 2, CRP 0.8. Lg1 antibodies none. There is no family history of chorea. Clonazepam did not help. Later, haloperidol did improve her chorea. Prednisone was stopped. MRI Brain 5 months later showed complete resolution of the hyperintensity in the putamen (Fig 3). Hba1c one year later is 5.4. The chorea partially improved. She requested to stop haloperidol and start valbenazine. Valbenazine did reduce the frequency and amplitude of the chorea, but caused somnolence.
Conclusion: The second hospitalization was associated with hemichorea, typical MRI findings for CHBG, and a normal serum glucose. Here, the chorea began 2 weeks before hospital evaluation. Recent glucose and Hba1c were quite high. MRI findings often persist for six months1. Literature search finds one other case report of CHBG syndrome associated with a normal glucose. In 2014, Bizet J et al reported a similar case2. While CHBG syndrome is usually seen with high serum glucose levels, this author similarly proposes that classic MRI findings and high Hba1c would be sufficient to consider CHBG.
References: 1. Chua CB, Sun CK, Hsu CW, Tai YC, Liang CY, Tsai IT. “Diabetic striatopathy”: clinical presentations, controversy, pathogenesis, treatments, and outcomes. Sci Rep. 2020 Jan 31;10(1):1594. doi: 10.1038/s41598-020-58555-w. PMID: 32005905; PMCID: PMC6994507. 2. Bizet J, Cooper CJ, Quansah R, Rodriguez E, Teleb M, Hernandez GT. Chorea, Hyperglycemia, Basal Ganglia Syndrome (C-H-BG) in an uncontrolled diabetic patient with normal glucose levels on presentation. Am J Case Rep. 2014 Apr 7;15:143-6. doi: 10.12659/AJCR.890179. PMID: 24744820; PMCID: PMC3989942.
To cite this abstract in AMA style:
M. Wangsuwana. Case of Chorea Hyperglycemia Basal Ganglia syndrome with normal glucose [abstract]. Mov Disord. 2021; 36 (suppl 1). https://www.mdsabstracts.org/abstract/case-of-chorea-hyperglycemia-basal-ganglia-syndrome-with-normal-glucose/. Accessed August 2, 2026.« Back to MDS Virtual Congress 2021
MDS Abstracts - https://www.mdsabstracts.org/abstract/case-of-chorea-hyperglycemia-basal-ganglia-syndrome-with-normal-glucose/