Category: Choreas (Non-Huntington's Disease)
Objective: To describe a patient who presented with hyperkinetic movements due to zoledronic acid-induced autoimmunity.
Background: Chorea is a rare neurologic manifestation of antiphospholipid syndrome (APS). APS is theorized to be due to pathogenic antibodies that gain access to the CNS through disruption of the blood brain barrier [1]. Bisphosphonates have previously been reported to induce a systemic inflammatory response and present as conditions including autoimmune hepatitis, rheumatoid arthritis, polymyalgia rheumatica, and Crohn’s disease flare [2,3].
Method: We describe the clinical presentation of an autoimmune movement disorder with a novel etiology.
Results: A 71-year-old female with a history of breast cancer in remission presented one month following zoledronic acid administration with involuntary leg movements and gait instability that progressed to violent large-amplitude choreo-ballistic movements in her lower more than upper extremities and orofacial dyskinesias. Due to the severity of the hyperkinetic movements, she required intubation for airway protection. Workup revealed normal serum calcium, copper, inflammatory markers, and thyroid levels. CSF cell count, protein and cultures were normal, and CSF autoimmune/paraneoplastic movement disorders panel was negative. The initial MRI brain showed acute infarcts in the right motor strip, with interval development of tiny bilateral infarcts on repeat MRI [figure 1]. Subsequent serologic studies were notable for positive ANA titer and with elevated beta-2-glycoprotein, anti-cardiolipin, and antiphospholipid antibodies consistent with APS.
The patient was initiated on intravenous heparin for APS, but subsequently developed heparin-induced thrombocytopenia so was transitioned to fondaparinux. She also received IV methylprednisolone 1g/kg for five days and underwent five sessions of plasmapheresis. Hyperkinetic movements improved with these therapies and symptomatic treatment with risperidone, clonazepam, and benztropine. She was then extubated and ultimately discharged with a slow oral prednisone taper and warfarin.
Conclusion: This case highlights a novel manifestation of bisphosphonate-induced autoimmunity. There is only one other report of a movement disorder following bisphosphonate administration which was ultimately attributed to hypocalcemia [4]. Increasing awareness can inform providers to recognize these rare reactions.
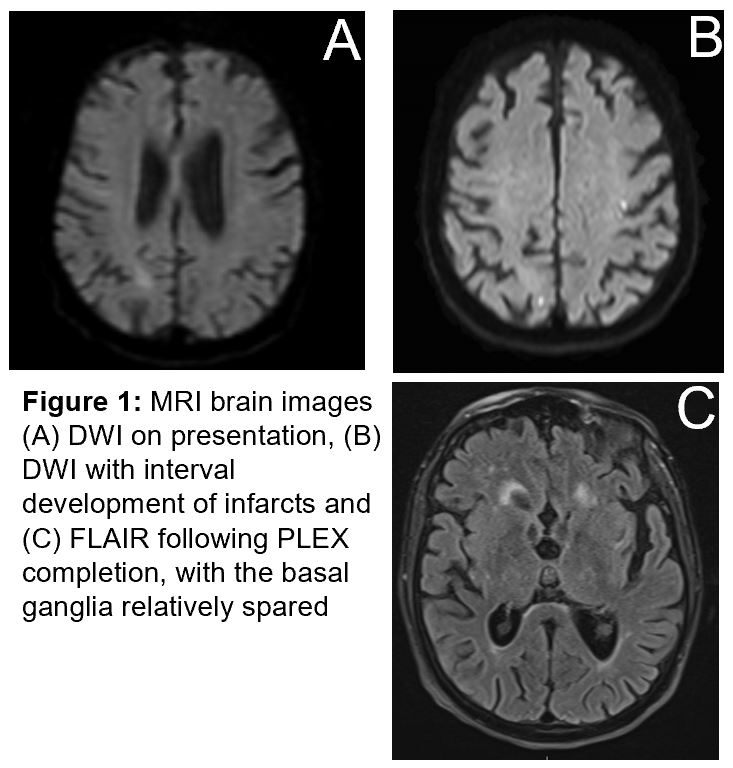
Figure 1
References: 1. Kyle, K., Bordelon, Y., Venna, N., & Linnoila, J. (2022). Autoimmune and Paraneoplastic Chorea: A Review of the Literature. Frontiers in Neurology, 13, 829076. https://doi.org/10.3389/fneur.2022.829076.
2. Jamil, M., Daneshvar, A., Nachawati, D., El Sharu, H., & Meysami, A. (2023). A Rare Presentation of Zoledronate-Induced Systemic Inflammatory Response. Cureus, 15(7), e41524. https://doi.org/10.7759/cureus.41524
3. Markovits, N., Loebstein, R., & Bank, I. (2017). Immune-mediated syndromes following intravenous bisphosphonate therapy. Inflammopharmacology, 25(6), 665–671. https://doi.org/10.1007/s10787-017-0365-9
4. Topakian, R., Stieglbauer, K., Rotaru, J., Haring, H. P., Aichner, F. T., & Pichler, R. (2006). Hypocalcemic choreoathetosis and tetany after bisphosphonate treatment. Movement Disorders : Official Journal of the Movement Disorder Society, 21(11), 2026–2027. https://doi.org/10.1002/mds.21094
5. Leistikow, P., Joseph, N., Shah-Zamora, D. (2024, February 23-25). Choreoballism due to Bisphosphonate-Induced Antiphospholipid Syndrome: A Case Report. [Conference Presentation]. Greensboro, NC, United States.
To cite this abstract in AMA style:
P. Leistikow, N. Joseph, D. Shah-Zamora. Choreoballism due to Bisphosphonate-Induced Antiphospholipid Syndrome: A Case Report [abstract]. Mov Disord. 2024; 39 (suppl 1). https://www.mdsabstracts.org/abstract/choreoballism-due-to-bisphosphonate-induced-antiphospholipid-syndrome-a-case-report/. Accessed August 8, 2026.« Back to 2024 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/choreoballism-due-to-bisphosphonate-induced-antiphospholipid-syndrome-a-case-report/