Session Information
Date: Saturday, October 6, 2018
Session Title: Rare Genetic and Metabolic Diseases
Session Time: 1:45pm-3:15pm
Location: Hall 3FG
Objective: We report a patient with stable neurological Wilson disease (WD) who developed repeated seizures and new-onset cortical-subcortical lesions, and discuss the possible causes for the changes.
Background: Cortical-subcortical lesions and seizures have been reported in 5-10% and 4-8% of patients with WD respectively, and are often observed concurrently. However, their occurrence in a stable patient on treatment has not been reported.
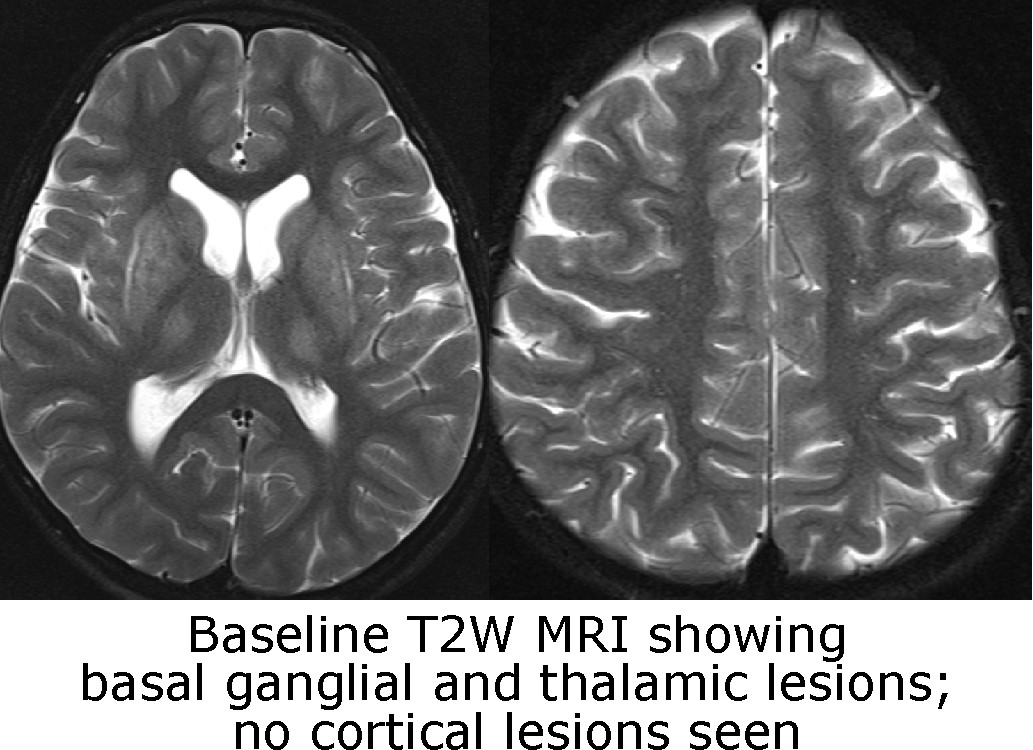
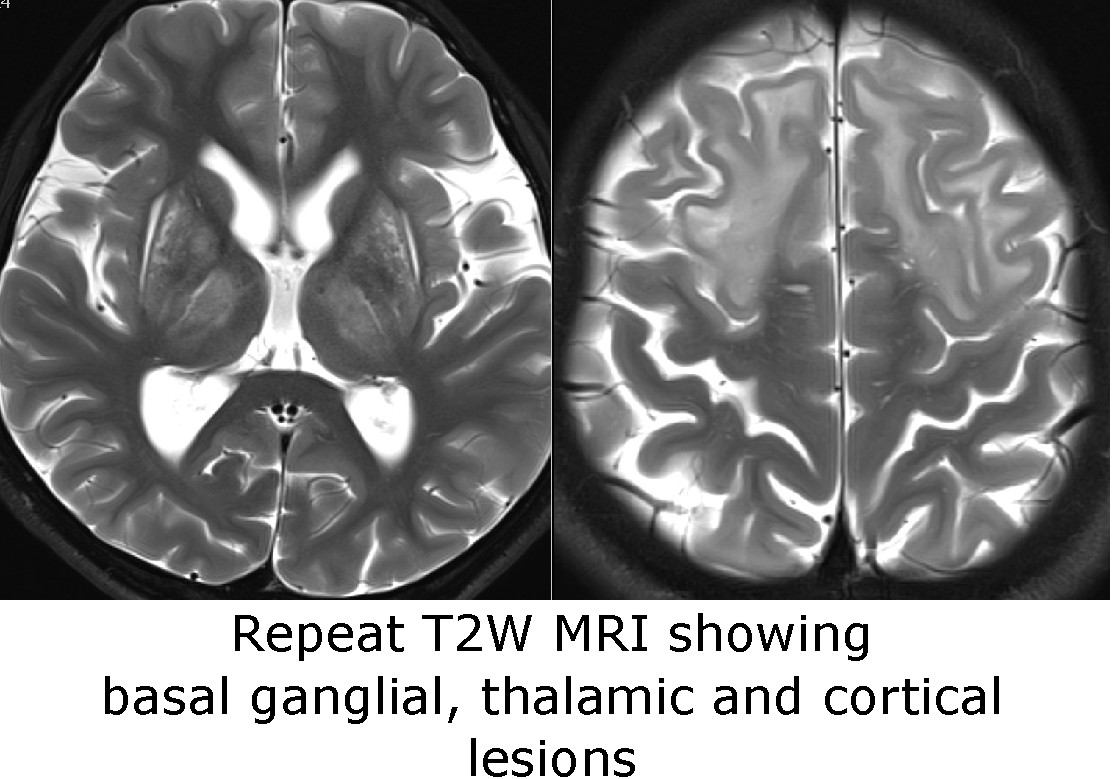
Methods: An eight year old boy developed progressive dysarthria, gait imbalance and behavioral changes over 18 months. Examination also showed Kayser-Fleischer rings, Wilsonian faces, and generalized dystonia. He could walk independently and maintain high grades at school. WD was diagnosed. T2W and FLAIR brain MRIs showed symmetrical basal ganglial and thalamic lesions; no cortical lesions were present [figure1]. With copper chelation (penicillamine gradually escalated from 125mg/d to 1g/d) there was significant neurological improvement over the next 10 months. At that point though he developed recurrent seizures; initially once every few weeks but, despite antiepileptics, increasing to multiple seizures per day after two months. He became dull, somnolent and unsteady. Repeat brain MRI a year after the first scan showed new-onset patchy lesions in the frontal and parietal cortical-subcortical areas [figure2]. Video EEG showed clinical and electrical frontal lobe seizures. Intravenous benzodiazepine and levetiracetam, and pulse methylprednisolone (to decrease cerebral inflammation), were administered and controlled the seizures promptly. Longer-term antiepileptic treatment was also intensified. Penicillamine was maintained at 1g/d. Cognition and balance recovered over the next few weeks.
Results: Very frequent or prolonged seizures (in diseases other than WD) have been shown to lead to acute postictal cortical lesions. Such changes are believed to result from seizure-induced neuronal hyperexcitation, increased cellular metabolic demand and sodium/potassium ATP pump failure. In WD, copper deposits in the cortical grey matter increase cellular metabolic stress. We hypothesise that repeated seizures heighten this stress markedly, precipitate cellular injury and death, and can lead to new-onset cortical-subcortical lesions and even induce further seizures.
Conclusions: Late-onset seizures and concurrent cortical lesions can develop in stable WD patients undergoing treatment. We hypothesize that the seizures may contribute to the development of the lesions. If true, this would suggest that prompt control of seizures can limit such cortical-subcortical lesions.
References: 1. Aggarwal A, Bhatt M. Neurological Wilson disease. In Kerkar N and Roberts EA, editors: Clinical and Translational Perspectives on Wilson Disease, Elsevier, 2018, in print. 2. Prashanth LK, Sinha S, Taly AB, Mahadevan A, Vasudev MK, Shankar SK. Spectrum of epilepsy in Wilson’s disease with electroencephalographic, MR imaging and pathological correlates. J Neurol Sci. 2010;291:44-51. 3. Moritani T, Smoker WR, Sato Y, Numaguchi Y, Westesson PL. Diffusion-weighted imaging of acute excitotoxic brain injury. AJNR Am J Neuroradiol. 2005;26:216-28.
To cite this abstract in AMA style:
A. Aggarwal, M. Munshi, P. Gadgil, D. Sanghvi, M. Bhatt. Explosive flurry of seizures and new-onset cortical-subcortical lesions in a patient with Wilson disease [abstract]. Mov Disord. 2018; 33 (suppl 2). https://www.mdsabstracts.org/abstract/explosive-flurry-of-seizures-and-new-onset-cortical-subcortical-lesions-in-a-patient-with-wilson-disease/. Accessed August 6, 2026.« Back to 2018 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/explosive-flurry-of-seizures-and-new-onset-cortical-subcortical-lesions-in-a-patient-with-wilson-disease/