Objective: To present movement disorder symptoms of Holmes tremor and dystonia as part of Benedikt Syndrome in a patient diagnosed with HIV-Related Cerebral Toxoplasmosis
Background: Neurological complications of HIV due to opportunistic infection, such as Cerebral Toxoplasmosis are common, yet troublesome. Toxoplasmosis is positively correlated with immunodeficiency status, marked by low CD4+ levels,[1] and can lead to intracranial pathology whose neurological disturbance is aligned with structural lesion, sometimes comply specific syndromes. Benedikt syndrome is a rare syndrome marked by ipsilateral oculomotor nerve palsy, contralateral hemiparesis, and contralateral movement disorder.[2] Holmes tremor manifested as rest, postural, and intention tremor, mainly secondary to lesion of the cerebello-thalamo-cortical or dentato-rubro-olivary tract involving midbrain, thalamus, and cerebellum.[3] Dystonia is sustained muscle contractions, causing twisting or abnormal postures, which is primary or secondary to the lesion of the nigrostriatal pathway.[4]
Method: A 25-year-old woman, came to ER with symptoms of decreased consciousness (GCS 12/15), right ophthalmoplegia, left half-body weakness, and involuntary movements. She had tremor in left forearm at rest, raising hand, reaching goal defined as Holmes tremor, and also an abnormal dystonic posture of left fingers.
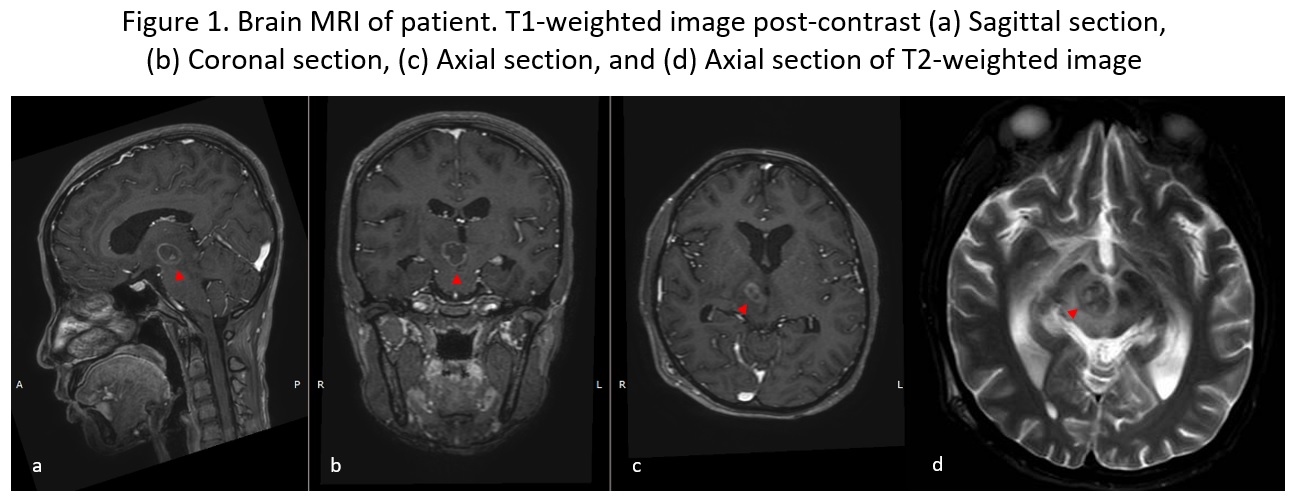
Results: Brain MRI showed lesions at the right thalamus, mesencephalon, and right pons, which is ipsilateral to oculomotor nerve palsy and contralateral to hemiparesis and movement disorder, supporting clinical criteria of Benedikt syndrome. She was HIV-positive with low CD4+ cell count of <50/mL and had raised IgG antibody levels of >650 U/mL. She was given toxoplasmosis therapy with pyrimethamine and clindamycin, antiretroviral therapy, and clonazepam as a treatment option for Holmes tremor and dystonia. The patient was discharged with GCS 15, and the latest 9-month follow-up showed improvement of motoric function and ophthalmoplegia, while movement disorders persist but qualitatively decreased.
[Figure1]
Conclusion: This case is essential to describe the clinical features of Benedict syndrome, implying intracranial pathology in HIV-positive people, mainly for cerebral toxoplasmosis. It also highlights that pharmacological treatment is usually impractical for Holmes tremor, although the etiological therapy was given properly.
References: 1. Munir, B., Rianawati, S. B. and Rosyid, H. Al (2020) ‘The comparison of cognitive function disorder before and after early therapy for cerebral toxoplasmosis in HIV/AIDS patients’, HIV and AIDS Review, 9(1), pp. 30–33. doi: 10.5114/hivar.2020.93159.
2. Burr P, Mandalaneni K. Benedikt Syndrome. [Updated 2022 Jul 5]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-
3. Hey, G. et al. (2022) ‘Evolving Concepts in Our Understanding and Treatment of Holmes Tremor, Over 100 Years in the Making’, Tremor and Other Hyperkinetic Movements, 12(1), pp. 1–12. doi: 10.5334/tohm.683.
4. Albanese, A. and Del Sorbo, F. (2016) ‘Dystonia and tremor: The clinical syndromes with isolated tremor’, Tremor and Other Hyperkinetic Movements, 2016, pp. 1–10. doi: 10.7916/D8X34XBM.
To cite this abstract in AMA style:
NER. Raisa, AC. Pratiwi, SB. Rianawati, BDM. Munir. Holmes Tremor and Dystonia as Manifestation of Benedikt Syndrome in HIV-Related Cerebral Toxoplasmosis : A Case Report [abstract]. Mov Disord. 2023; 38 (suppl 1). https://www.mdsabstracts.org/abstract/holmes-tremor-and-dystonia-as-manifestation-of-benedikt-syndrome-in-hiv-related-cerebral-toxoplasmosis-a-case-report/. Accessed June 21, 2026.« Back to 2023 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/holmes-tremor-and-dystonia-as-manifestation-of-benedikt-syndrome-in-hiv-related-cerebral-toxoplasmosis-a-case-report/