Objective: To compare literature data on psychogenic tremor and clinical and MRI data of the patient.
Background: Dystonia is a involuntary, sustained or repetitive, patterned muscle contractions or spasms, frequently causing squeezing, twisting and other movements or abnormal postures.Psychogenic dystonia can manifest as fixed or mobile dystonia [1].Psychogenic dystonia is characterized with 1) age at onset: second to fourth decade, 2) females suffer more frequent, 3)phenotypic:Lower limbs>upper limb >neck/shoulder; fixed plantar flexion and inversion with toe curling; carpal flexion with prominent clawing of fourth and fifth fingers; tonic dystonic posturing of neck (latero/torticollis), 4) additional features: absence of sensory tricks or overflow dystonia. [2,3].
Method: We present a clinical case of a patient of 14 years old, applied for an appointment at the Center for MDS, Kazan with acute hyperkinesis in the left arm, which became more pronounced within six months (“I used to be able to control”, reducing by “a certain position of the arm”; lately these tricks did not help), then the unvoluntary position of the left foot joined. The patient’s mother has been suffering from acute leukemia for two years before and the girl often has to be on duty at her mother’s hospital and hyperkinesis arose after another night shift with her mother in hematology. On examination, choreodistonic hyperkinesis in the left arm and dystonic position of the left foot (fixed plantar flexion and inversion with flexion of the toes on the left), flexion of the wrist with pronounced clawing of the fourth and fifth fingers; the absence of sensory tricks or overflow dystonia were observed. On the performed MRI (3 Tl) with angiography, revealed a giant arteriovenous malformation in the structure of the basal ganglia on the right.
Results: The patient underwent stereotactic radiosurgery to the target in the area of the basal ganglia of the right hemisphere with a reduction in the size of the vascular tangle of arteriovenous malformation with a slight regression of symptoms.
Conclusion: Even with great confidence of the doctor in the diagnosis of psychogenic motor disorder, additional diagnostic methods are necessary to exclude the organic nature of the disease.
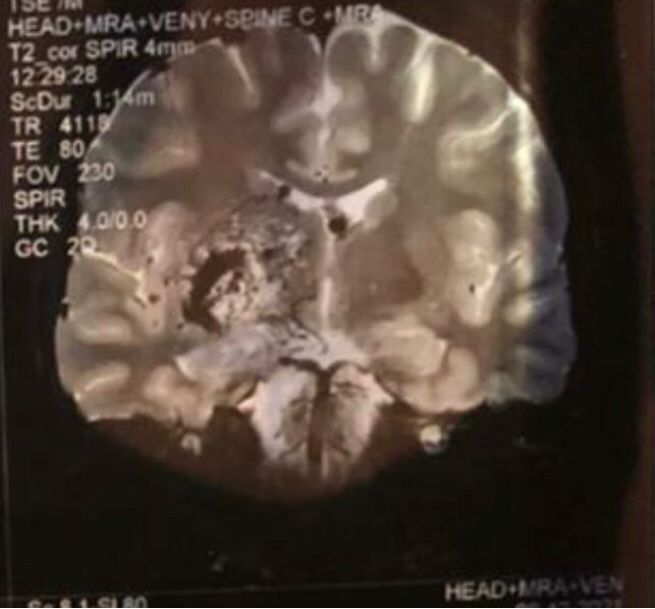
a giant arteriovenous malformation in right

a giant arteriovenous malformation right
References: 1. https://www.bcm.edu/healthcare/specialties/neurology/parkinsons-disease-and-movement-disorders/psychogenic-movement-disorders
2. Ganos C, Edwards MJ, Bhatia KP. The Phenomenology of Functional (Psychogenic) Dystonia. Mov Disord Clin Pract. 2014 Apr 10;1(1):36-44. doi: 10.1002/mdc3.12013. PMID: 30363921; PMCID: PMC6183180.
3. Tan EK, Jankovic J. Psychogenic hemifacial spasm. J Neuropsychiatry Clin Neurosci 2001;13:380–384. [PubMed] [Google Scholar]
To cite this abstract in AMA style:
G. Ilina, D. Khasanova, Z. Zalyalova, A. Lestrovaya. Is acute dystonia in a teenager psychogenic dystonia? [abstract]. Mov Disord. 2024; 39 (suppl 1). https://www.mdsabstracts.org/abstract/is-acute-dystonia-in-a-teenager-psychogenic-dystonia/. Accessed August 8, 2026.« Back to 2024 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/is-acute-dystonia-in-a-teenager-psychogenic-dystonia/