Session Information
Date: Wednesday, June 7, 2017
Session Title: Myoclonus
Session Time: 1:15pm-2:45pm
Location: Exhibit Hall C
Objective: Movement disorders in pregnancy represent a diagnostic challenge due to the poor physiopathological understanding in the extrapyramidal system where the afferent and efferent circuits in balance of voluntary movements undergo alterations apparently without a specific etiology. Psychogenic movements during the gestational stage tend to pose a diagnostic challenge that can be elucidated by performing an adequate examination, sometimes can to be a exclusion diagnosis due to a “uknown” prevalence found in the pregnant patient should be taken as part of the spreads within the spectrum of movement disorders.
Background: A 27-year-old female with a normal-evolutionary pregnancy of 23.2 gestational weeks with a history of intrafamily violence that presents acute and sudden synchronous abdominal movements, rhythmic, at rest, paroxysmal, triggered by abdominal palpation and noise, nocturnal, with 4 hrs evolution without aggregate gastrointestinal clinic that enters the emergency department.
Methods: The patient was approached where medical-surgical abdominal and obstetric emergency was ruled out; neurological examination showed suppression of movement with distraction, increased with attention, periodical, durtion of 90-seconds, Hamilton Scale test of 24 points revealed severe depression, psychological stimulus was a discussion hours prior to the onset of the symptomatology, rest of examination was normal.
Results: Basic biochemical serum controls within physiological parameters. Electroencephalogram without evidence of epileptic activity, somatosensory potentials of normal medial and tibial nerve, MRI of brain and cervical spine without evidence of lesion, electromyography of phrenic nerves and abdominal wall musculature were normal. The psychiatric profile and the sudden clinical features with emotional trigger were diagnosed as abdominal psychogenic myoclonus, concordant with the Fahn-Williams criteria, then behavioral psychotherapy was started, with remission of movement disorder.
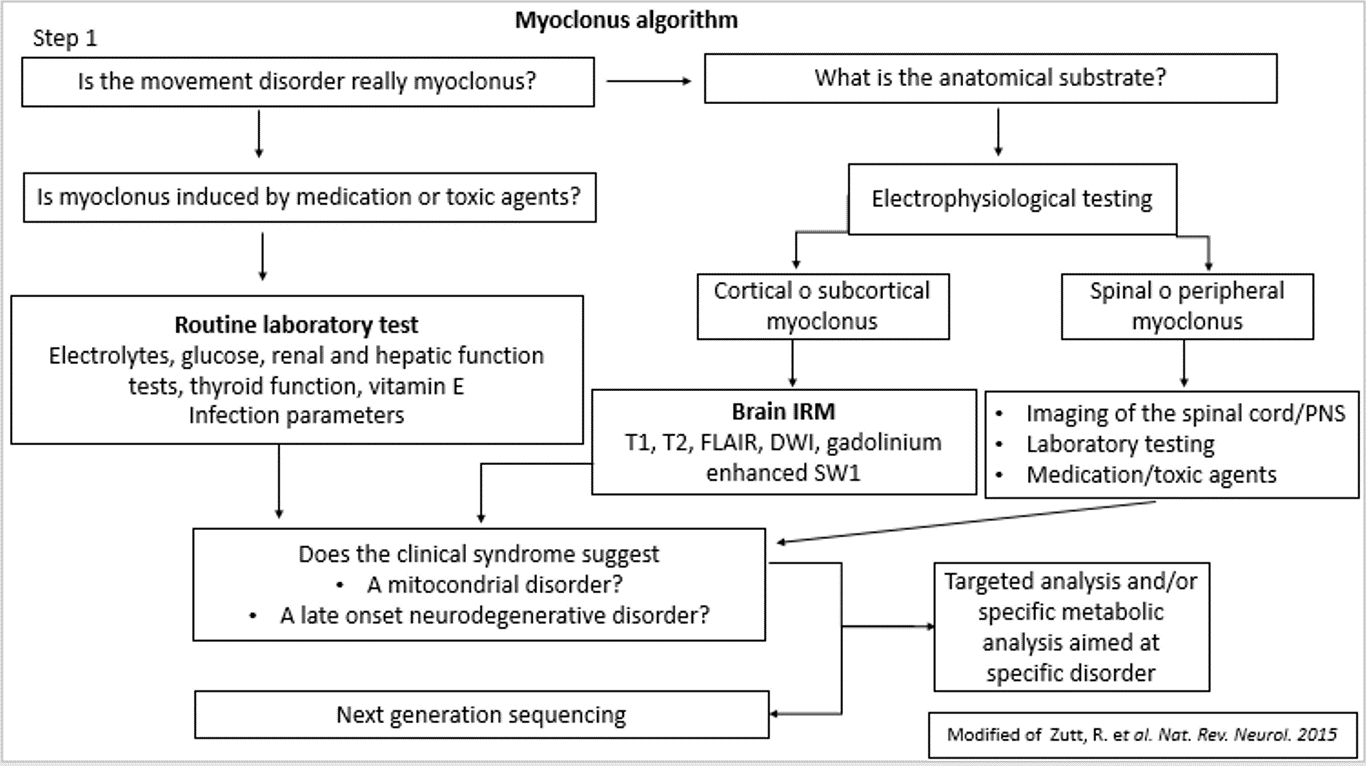

Conclusions: The psychogenic myoclonus is integrated, the diagnostic algorithm of Zutt et al was an angular tool to perform the approach, physiopathologically these disorders do not have a well-founded anatomical substrate although with a psychiatric phenotype that may help to make such a diagnosis classically considered as exclusion. Due to the obstetric situation, this patient could not have pharmacological treatment because of the high teratogenic potential.
References: MJ Edwards, KP Bhatia. Functional (psychogenic) movement disorders: merging mind and brain. Lancet Neurol 2012; 11: 250–60.
JM Miyasaki, A AlDakheel. Movement Disorders in Pregnancy. Continuum (Minneap Minn) 2014;20(1):148–161.
R Zutt, ME Van Egmond, JW Elting et al. A novel diagnostic approach to patients with myoclonus. Nat. Rev. Neurol 2015; 198: 1-11.
F Morgante, MJ Edwards, AJ Espay. Continuum (Minneap Minn) 2013;19(5):1383–1396.
To cite this abstract in AMA style:
D. García, P.O. Vargaz, Z. Lopez. Psychogenic abdominal myoclonus in Pregnancy: Case Report [abstract]. Mov Disord. 2017; 32 (suppl 2). https://www.mdsabstracts.org/abstract/psychogenic-abdominal-myoclonus-in-pregnancy-case-report/. Accessed August 5, 2026.« Back to 2017 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/psychogenic-abdominal-myoclonus-in-pregnancy-case-report/