Category: Rare Genetic and Metabolic Diseases
Objective: We present a case series of movement disorders associated with vitamin B12 deficiency
Background: Vitamin B12 deficiency can cause multiple neuropsychiatric disorders like peripheral neuropathy, myelopathy, myeloneuropathy, dementia, cerebellar ataxia, optic neuropathy, psychosis, mood and personality disturbances.1 Various types of movement disorders have been described in vitamin B12 deficiency. Vitamin B12 deficiency can present as infantile tremor syndrome. Cerebellar ataxia and extrapyramidal manifestations like chorea, dystonia, and parkinsonism have been infrequently described in adults with vitamin B12 deficiency.2 We present a case series of movement disorders associated with vitamin B12 deficiency.
Method: We present a case series of four patients with movement disorders associated with vitamin B12 deficiency. We retrospectively assessed the patients admitted at Institute of Medical Sciences and SUM Hospital in India, who had movement disorders related to Vitamin B12 deficiency. All the clinical details, phenomenology, laboratory parameters and imaging parameters were assessed.
Results: Mean age of presentation was 55 year (range 44 to 76 years). Three patients were pure vegetarian and one patient was on mixed diet. Two patients were wheel chair bound with gross sensory ataxia, pseudoathetosis and pseudodystonia at presentation. One patient had pseudoathetosis with peripheral neuropathy with minimal sensory ataxia. One patient had presentation in form of parkinsonism and sensory ataxia. The mean duration of symptoms at presentation was 80 days (range 20 days to 180 days). All the 4 patients had low vitamin B12 of 70 pg/ml (range-50-104). The mean MCV was 115 fl (range-104-125). Serum homocysteine was elevated in three patients with mean homocysteine of 137 micromole/l (range-44-308). One patient with gross sensory ataxia, who was on mixed diet was positive for Anti Intrinsic factor antibody. MRI Spine of three patients showed T2/FLAIR hyperintense signal in the dorsal aspect of spinal cord. All patients were treated with injectable methylcobalamine. All three patients with sensory ataxia and pseudoathetosis had significant improvement. The patient with parkinsonism didn’t have significant improvement.
Conclusion: In India, where most people are vegetarian because of spiritual and cultural reasons, vitamin B12 deficiency may be considered, as treatment is simple, and patient can get complete recovery.
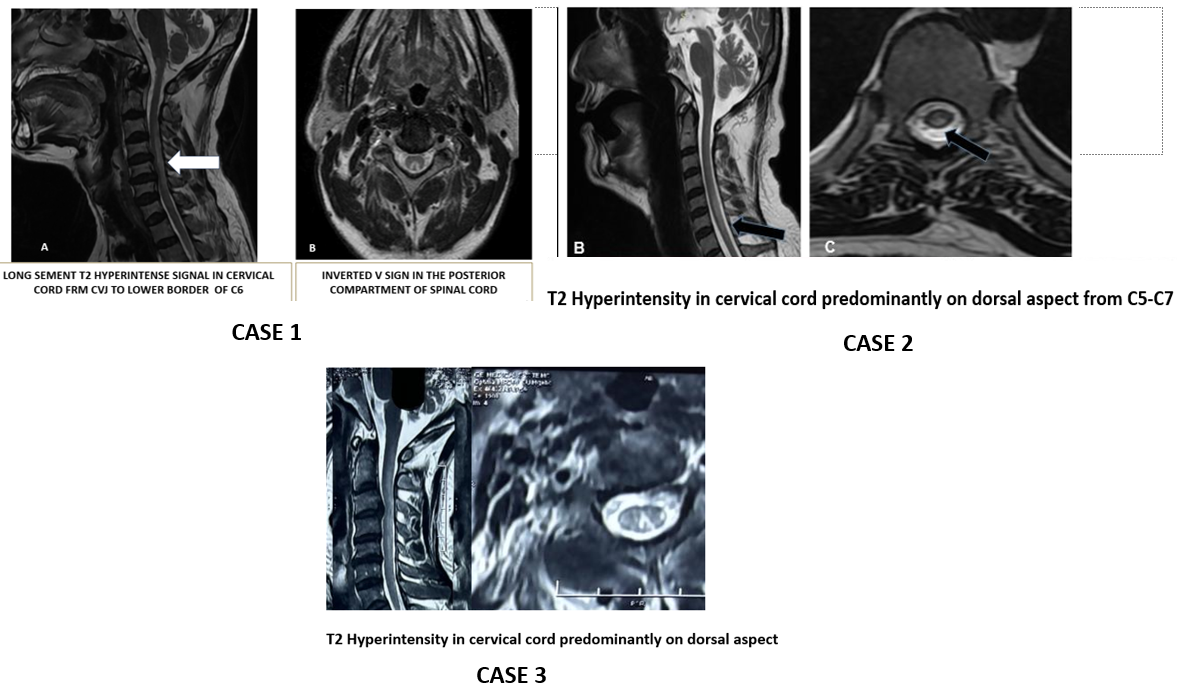
MRI CERVICAL SPINE
References: 1. Healton EB, Savage DG, Brust JC, Garrett TJ, Lindenbaum J. Neurologic aspects of cobalamin deficiency. Medicine (Baltimore). 1991 Jul;70(4):229-45.
2. Shyambabu C, Sinha S, Taly AB, Vijayan J, Kovoor JM. Serum vitamin B12 deficiency and hyperhomocystinemia: a reversible cause of acute chorea, cerebellar ataxia in an adult with cerebral ischemia. J Neurol Sci. 2008 Oct 15;273(1-2):152-4
To cite this abstract in AMA style:
L. Sahoo, A. Mishra, D. Dash, M. Karan. Spectrum of Movement Disorders in Vitamin B12 Deficiency: A Case Series from India [abstract]. Mov Disord. 2024; 39 (suppl 1). https://www.mdsabstracts.org/abstract/spectrum-of-movement-disorders-in-vitamin-b12-deficiency-a-case-series-from-india/. Accessed July 4, 2026.« Back to 2024 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/spectrum-of-movement-disorders-in-vitamin-b12-deficiency-a-case-series-from-india/