Objective: To describe two hyperkinetic disorders with manifestations that support the description of stiff-person syndrome
Background: Stiff-person syndrome (SPS) is a rare condition with just 1-2 cases per million people. The majority of cases affect individuals between the ages of 20 and 50, and the majority are female (3:1). Clinically, it shows up as stiffness, lumbar hyperlordosis, or muscle pain [2]. Patients may also experience additional neurological symptoms, such as myoclonus, problems with eye movement, and neuropsychiatric symptoms, which can result in a misdiagnosis of a functional neurological disorder (FND) [3]. A comprehensive clinical history and neurological exam are necessary in order to follow the proper diagnosis pathway.
Method:
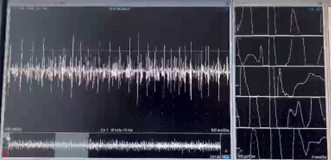
We discuss two cases of patients who were admitted at the National Institute of Neurology and Neurosurgery, as well as the final diagnosis established after work-up testing. The first patient is a 35-year-old woman. During a family discussion, she suddenly developed lumbar muscular discomfort. She also showed periods of anguish and uncontrollable crying. She demonstrated hyperlordosis during the examination as well as inconsistent, hyperkinetic lumbar muscle movements that fluctuated and decreased with distraction [figure1].
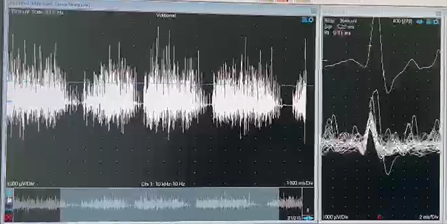
The second patient is a 58-year-old male. He first experienced sporadic, increasing lumbar pain. He showed uncontrolled axial movement spasms during the following two months, along with fatigue and diaphoresis. He revealed abnormal mental status, aberrant eye movement, hyperlordosis, and hypertrophy of the paraspinal muscles upon examination [figure 2].
Results: Serum GAD-65 levels were negative in both cases. Neurophysiological tests on both individuals exhibited abnormal results, with continuous myogenic activity seen in the thoracic and lumbar paraspinal muscles. Antagonist muscles did not exhibit any activation.
The female patient was diagnosed with a FND based on the variability of her symptoms and the improvement with distraction. The male patient, was treated for SPS with an intravenous immunoglobulin course of 2 g/kg divided into five days and clonazepam, with improvement of the symptoms.
Conclusion: The stiff-man syndrome is a clinical diagnosis challenge, even though there are established diagnostic criteria. To make the correct diagnosis, we must be aware of and sensitive to the subtle signs and symptoms of this disorder



References: 1. Baizabal-Carvallo JF, Jankovic J. Stiff-person syndrome: insights into a complex autoimmune disorder. J Neurol Neurosurg Psychiatry. 2015 Aug;86(8):840-8. doi: 10.1136/jnnp-2014-309201. Epub 2014 Dec 15. PMID: 25511790.
2. Scott D. Newsome, Tory Johnson. Stiff person syndrome spectrum disorders; more than meets the eye. Journal of Neuroimmunology, Volume 369, 2022, 577915, ISSN 0165-5728,
3. Budhram A, Sechi E, Flanagan EP, et al. Clinical spectrum of high-titre GAD65 antibodies. Journal of Neurology, Neurosurgery & Psychiatry 2021;92:645-654
To cite this abstract in AMA style:
J. Garcia, S. Mireles, Y. Martinez, A. Alcocer. Stiff person syndrome vs functional neurological disorder: two patients with hyperkinetic movement disorder [abstract]. Mov Disord. 2023; 38 (suppl 1). https://www.mdsabstracts.org/abstract/stiff-person-syndrome-vs-functional-neurological-disorder-two-patients-with-hyperkinetic-movement-disorder/. Accessed August 2, 2026.« Back to 2023 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/stiff-person-syndrome-vs-functional-neurological-disorder-two-patients-with-hyperkinetic-movement-disorder/