Session Information
Date: Wednesday, June 22, 2016
Session Title: Clinical Phenomenology and Rating Scales
Session Time: 12:00pm-1:30pm
Objective: To use movement disorder (MD) expert analysis of phenomenology to provide a comprehensive evaluation of the MD associated with NMDA receptor-antibody encephalitis (NMDAR-AbE).
Background: NMDAR-AbE is frequent cause of autoimmune encephalitis. Encephalopathy with psychiatric features and a prominent MD prompt recognition of this disorder. Timely diagnosis is key as patients benefit from early immunotherapy. Although the presence of the MD is well documented, its phenomenology and differential diagnosis have not been systematically analysed.
Methods: Seven MD experts (KB, VF, MT, AL, TL, NN and KS) independently rated 76 anonymised videos of 37 patients with NMDAR-AbE and MD. They were blinded to diagnosis. A glossary of terms was agreed in advance. Experts used a standardised format to evaluate ‘dominant’ or ‘associated’ MD phenomenologies, affected body regions, and three differential diagnoses.
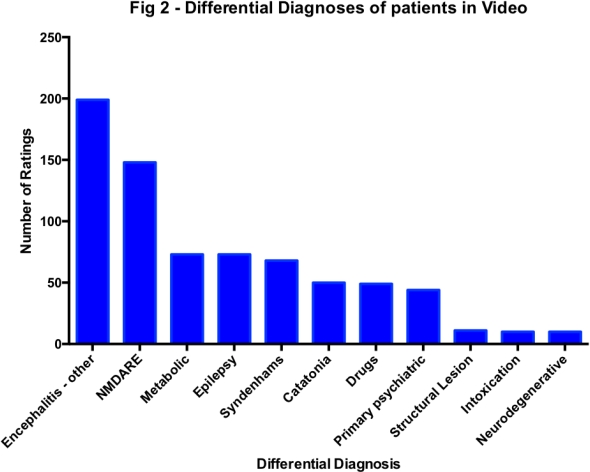
Results: The 76 videos attracted a total number of 932 dominant and associated MD ratings, a mean of 12 per video (range 5-24). Hyperkinetic MDs were observed most frequently (see fig 1), especially dystonia (23%), stereotypies (16%) and chorea (19%). The next most common phenomenologies included ballism (6%), myoclonus (6%) and clonic perseveration (7%). Hypokinetic disorders including bradykinesia and catatonia were seen with similar frequency (7% and 4%, respectively). Furthermore, these data allowed for observations to be made regarding inter-rater agreement, the relationships between phenomenologies and body parts involved. Facial movements, particularly characteristic of NMDAR-AbE, were described as predominantly choreiform with associated bradykinesia and stereotypies. NMDAR-AbE was listed as a differential diagnosis only 13% of the time, with the remainder described in alternative ways, most commonly encephalitis of other aetiology, metabolic disease and epilepsy (see fig 2). 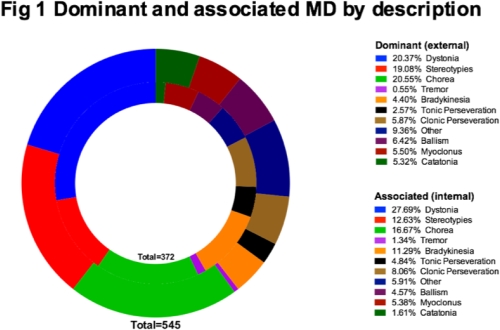
Conclusions: The MD associated with NMDAR-AbE is complex and predominantly hyperkinetic, with chorea, dystonia and stereotypies, strongly suggesting basal ganglia pathology. The complex and varied designations proposed by MD experts suggest that this disorder is unusually difficult to characterise and heterogeneous between patients. The interrelationships between various phenomenologies offer insights into more specific neural networks and further experiments should aim to understand the mechanisms of this unique pathophysiology.
To cite this abstract in AMA style:
J.A. Varley, K.P. Bhatia, R.C. Dale, V. Fung, T. Granata, M.A.J. Tijssen, A. Lang, J.P. Lin, M. Lim, T. Lynch, N. Nardocci, K.D. Sethi, S.R. Irani. The movement disorder associated with NMDAR-antibody encephalitis: An expert-rater video study [abstract]. Mov Disord. 2016; 31 (suppl 2). https://www.mdsabstracts.org/abstract/the-movement-disorder-associated-with-nmdar-antibody-encephalitis-an-expert-rater-video-study/. Accessed August 9, 2026.« Back to 2016 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/the-movement-disorder-associated-with-nmdar-antibody-encephalitis-an-expert-rater-video-study/