Category: Parkinsonism, Others
Objective: To present a rare case of asymmetric Parkinson disease (PD) due to a secondary structural lesion.
Background: PD is a neurodegenerative disease characterized by a slowly progressive and asymmetric parkinsonian syndrome. Although PD is the most common cause of asymmetric parkinsonian syndromes, its diagnosis relies heavily on clinical diagnosis and there is no consensus on the need for initial imaging study to rule out structural lesions.
Method: Case report and literature review.
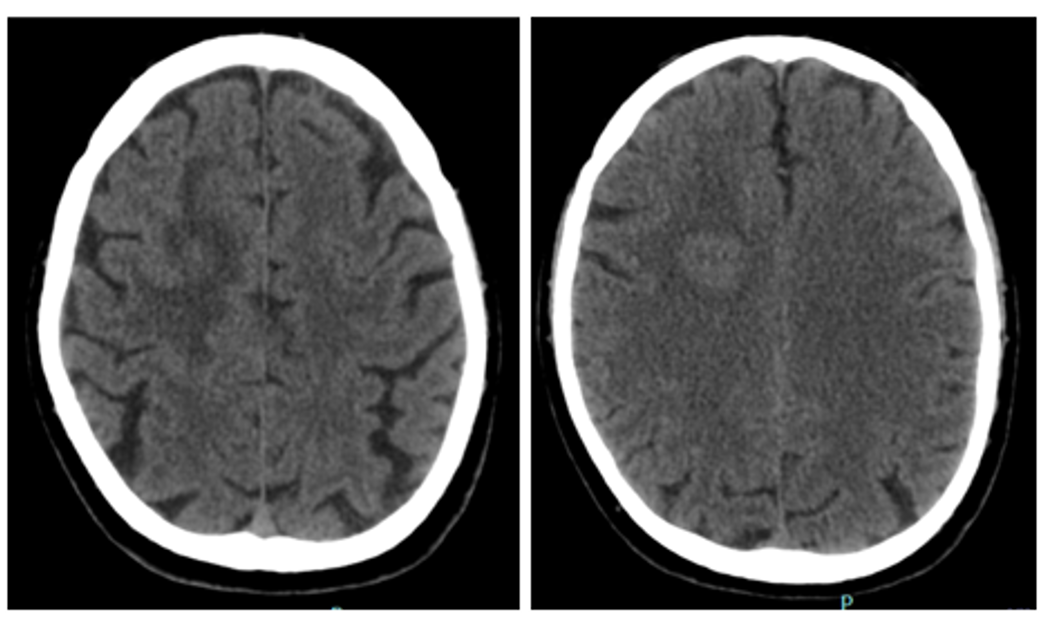
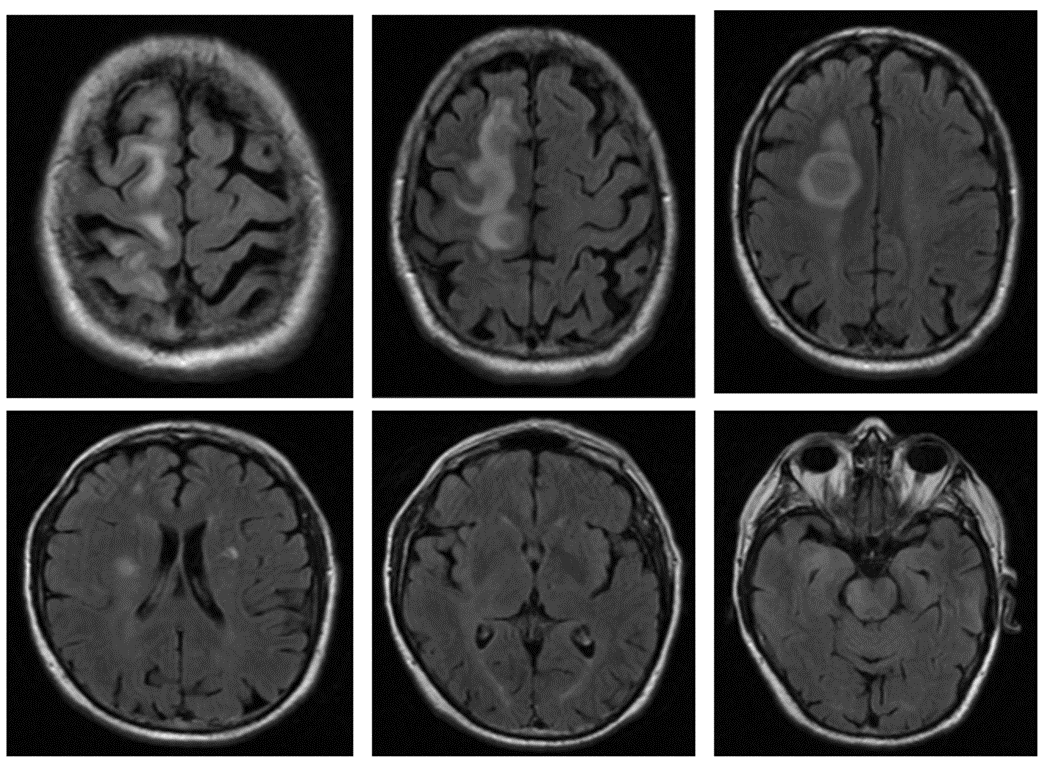
Results: A 72-year-old male was admitted to the Emergency Department due to imbalance, often leaning to the right in the previous 2 weeks, leading to two falls. He also reported asthenia and anorexia, starting three months prior to admission. His evaluation was striking for global bradikinesia with reduced eye blinking, rigidity in the left wrist associated with upper limb bradikinesia. He had diminished left arm swing, shorter stride and multiple steps when turning, there was no postural instability; the exam was otherwise unremarkable. CT-scan showed a right parietal hypodense space-occupying lesion [figure 1]. The latter MRi revealed multiple cortico-subcortical right frontal and parietal contrast-enhancing nodular lesions with centrum semiovale and corona radiata involvement with vasogenic edema. We found no evidence of extra-CNS primary neoplastic lesions [figure 2]. The patient underwent cerebral biopsy which showed a multiforme glioblastoma, IDH wild-type. He was referred for treatment with chemo- and radiation therapy, but unfortunately died within 1 month of the presentation at our department.
Conclusion: We report a case of a patient with a primary CNS neoplasm that presented with an asymmetric parkinsonian syndrome, mimicking a PD. We found few cases in the literature of parkinsonian syndromes associated with brain tumors. These occurred in several topographies, including outside the nigrostriatal path, such as thalamus and cingulate cortex [1,2]. With this case we aim to highlight the role of imaging studies in the initial work-up of asymmetric parkinsonian syndromes, especially rigid-akinetic type, and the “not to miss” differential diagnosis.
References: [1] Yasuhara, T. et al (2009). Parkinsonism related to brain tumors: a case report and review of the literature. The Open Neurosurgery Journal, 2(1).
[2] Höllerhage, M. (2019). Secondary parkinsonism due to drugs, vascular lesions, tumors, trauma, and other insults. International review of neurobiology, 149, 377-418.
To cite this abstract in AMA style:
P. Ferreira, R. Rocha, V. Carvalho. To scan or not to scan? Parkinsonian syndrome due to supratentorial glioblastoma [abstract]. Mov Disord. 2022; 37 (suppl 2). https://www.mdsabstracts.org/abstract/to-scan-or-not-to-scan-parkinsonian-syndrome-due-to-supratentorial-glioblastoma/. Accessed July 5, 2026.« Back to 2022 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/to-scan-or-not-to-scan-parkinsonian-syndrome-due-to-supratentorial-glioblastoma/