Session Information
Date: Sunday, October 7, 2018
Session Title: Parkinsonism, MSA, PSP (Secondary and Parkinsonism-Plus)
Session Time: 1:45pm-3:15pm
Location: Hall 3FG
Objective: To determine if 18F-FDG PET can differentiate Parkinson’s Disease from Parkinson’s-Plus syndromes
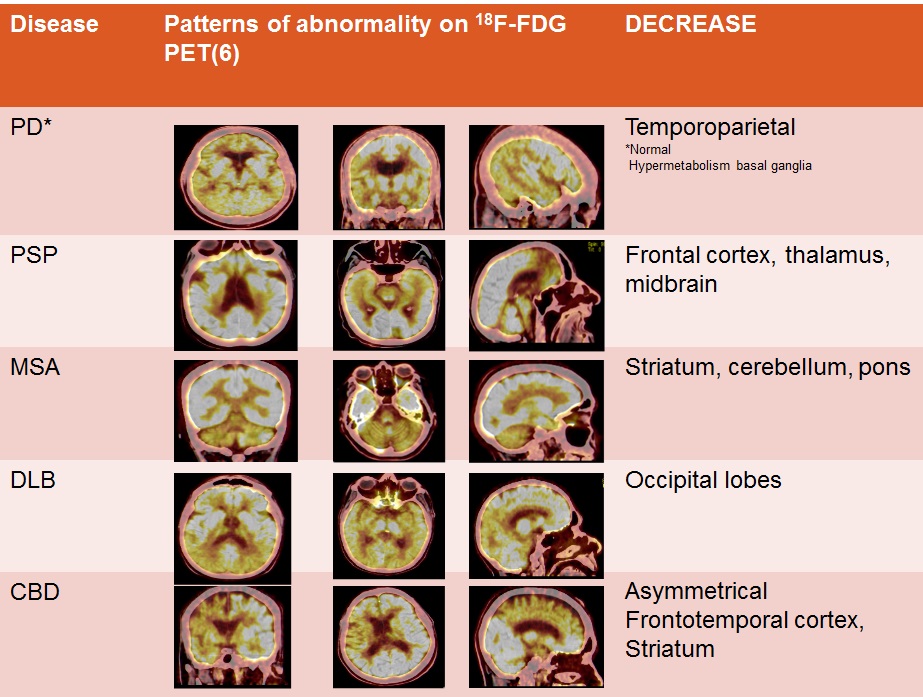
Background: Parkinsonism is a clinical syndrome of tremor, rigidity, bradykinesia and postural instability. PD is the commonest cause of parkinsonism. The other neurodegenerative causes are Multiple Systems Atropy (MSA), Progressive Supranuclear Gaze Palsy (PSP), Dementia with Lewy Bodies and Corticobasal Degeneration (CBD). These are known as the Parkinson’s -Plus syndromes (PPS). These forms of parkinsonism do not respond well to therapy and are associated with a poorer prognosis. Differentiating PD from PPS is therefore vital. However, two pathological studies have shown that the diagnostic accuracy of PD is only 76%. Movement disorder services improve the diagnostic accuracy of PD with a positive predictive value of 99%, however these services are not readily available and a marker for differentiating PD from PPS is required. A number of studies have used 18F-FDG PET to differentiate PD from PPS.
Methods: Patients with parkinsonism seen at the Neurology department from 2007-2017 who had an 18F-FDG PET were included in the study. All patients were given an 18F-FDG PET diagnosis by a Nuclear Medicine physician blinded to the clinical diagnosis. The criteria for disease related metabolic patterns was based on Eidelberg et al (1994). [Figure 1]. This was compared to a final clinical diagnosis diagnosis by a Neurologist in the Movement Disorder Service. Sensitivity, specificity, positive and negative predictive values were calculated. Our Neurology services are at a Tertiary Hospital in Durban, South Africa with a population of 11 million persons. Levodopa was withheld for 12 hours prior to 18F-FDG PET.
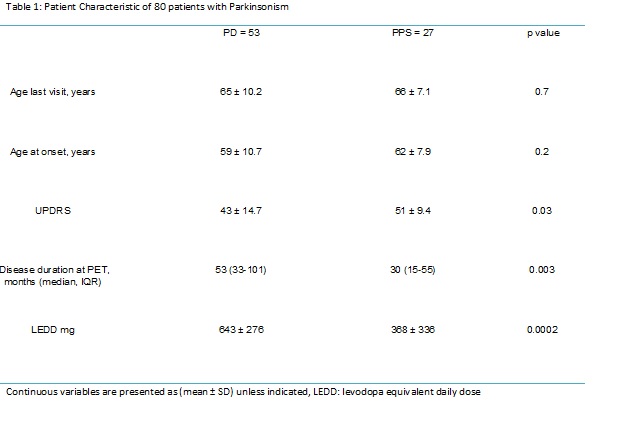
Results: 80 patients were included in the study, 53 had PD and 27 had PPS (10 PSP, 7 MSA, 8 DLB and 2 CBD). 18F-FDG PET diagnosis of the 53 PD patients: 48 were diagnosed as PD, 1 DLB, 2 MSA, 1 was given the diagnosis Frontotemporal Dementia on PET scan and 1 patient was diagnosed as HIV associated neurocognitive disorder. 18F-FDG PET diagnosis of the 27 PPS: 24 patients were correctly diagnosed and classified by 18F-FDG PET and 3 PPS patients were misdiagnosed as PD. Table 1 shows the characteristics of the 80 patients with parkinsonism. Patients with PPS had a higher UPDRS score with a shorter disease duration and used a lower dose of levodopa compared to PD patients. Table 2 shows the results of the patients.
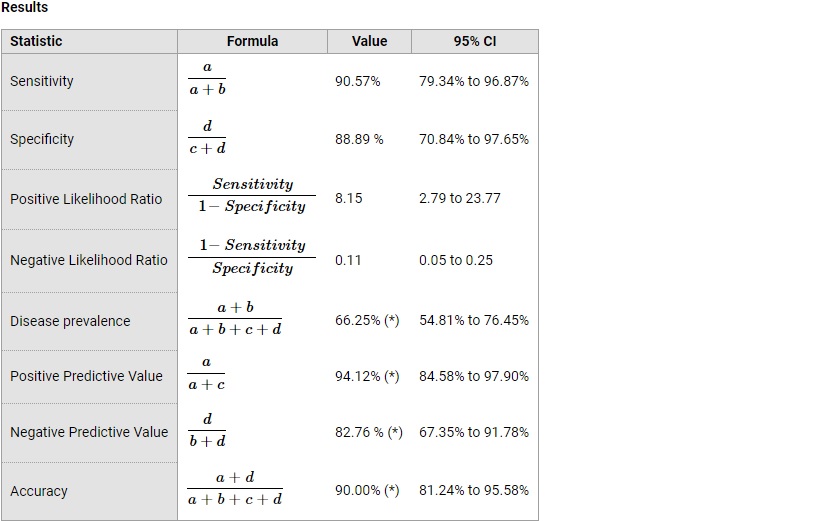
Conclusions: 18F-FDG PET can differentiate PD from PPS with an accuracy of 90%.
References: 1. Berti, V., L. Mosconi, and A. Pupi, Brain: normal variations and benign findings in fluorodeoxyglucose-PET/computed tomography imaging. PET Clin, 2014. 9(2): p. 129-40. 2. Brown, R.K., et al., Brain PET in suspected dementia: patterns of altered FDG metabolism. Radiographics, 2014. 34(3): p. 684-701. 3. Eckert, T., et al., FDG PET in the differential diagnosis of parkinsonian disorders. Neuroimage, 2005. 26(3): p. 912-21. 4. Hughes, A.J., et al., The accuracy of diagnosis of parkinsonian syndromes in a specialist movement disorder service. Brain, 2002. 125(Pt 4): p. 861-70. 5. Hughes, A.J., et al., Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: a clinico-pathological study of 100 cases. J Neurol Neurosurg Psychiatry, 1992. 55(3): p. 181-4. 6. Litvan, I., Recent advances in atypical parkinsonian disorders. Curr Opin Neurol, 1999. 12(4): p. 441-6. 7. Meyer, P.T., et al., (18)F-FDG PET in Parkinsonism: Differential Diagnosis and Evaluation of Cognitive Impairment. J Nucl Med, 2017. 58(12): p. 1888-1898.
To cite this abstract in AMA style:
F. Amod. 18F-FDG PET brain in Parkinsonism [abstract]. Mov Disord. 2018; 33 (suppl 2). https://www.mdsabstracts.org/abstract/18f-fdg-pet-brain-in-parkinsonism/. Accessed July 13, 2026.« Back to 2018 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/18f-fdg-pet-brain-in-parkinsonism/