Category: Parkinsonism, Others
Objective: We discuss a patient with rapidly progressive parkinsonism with radiological features of normal pressure hydrocephalus, who was diagnosed with obstructive hydrocephalus secondary to intracranial metastatic deposits.
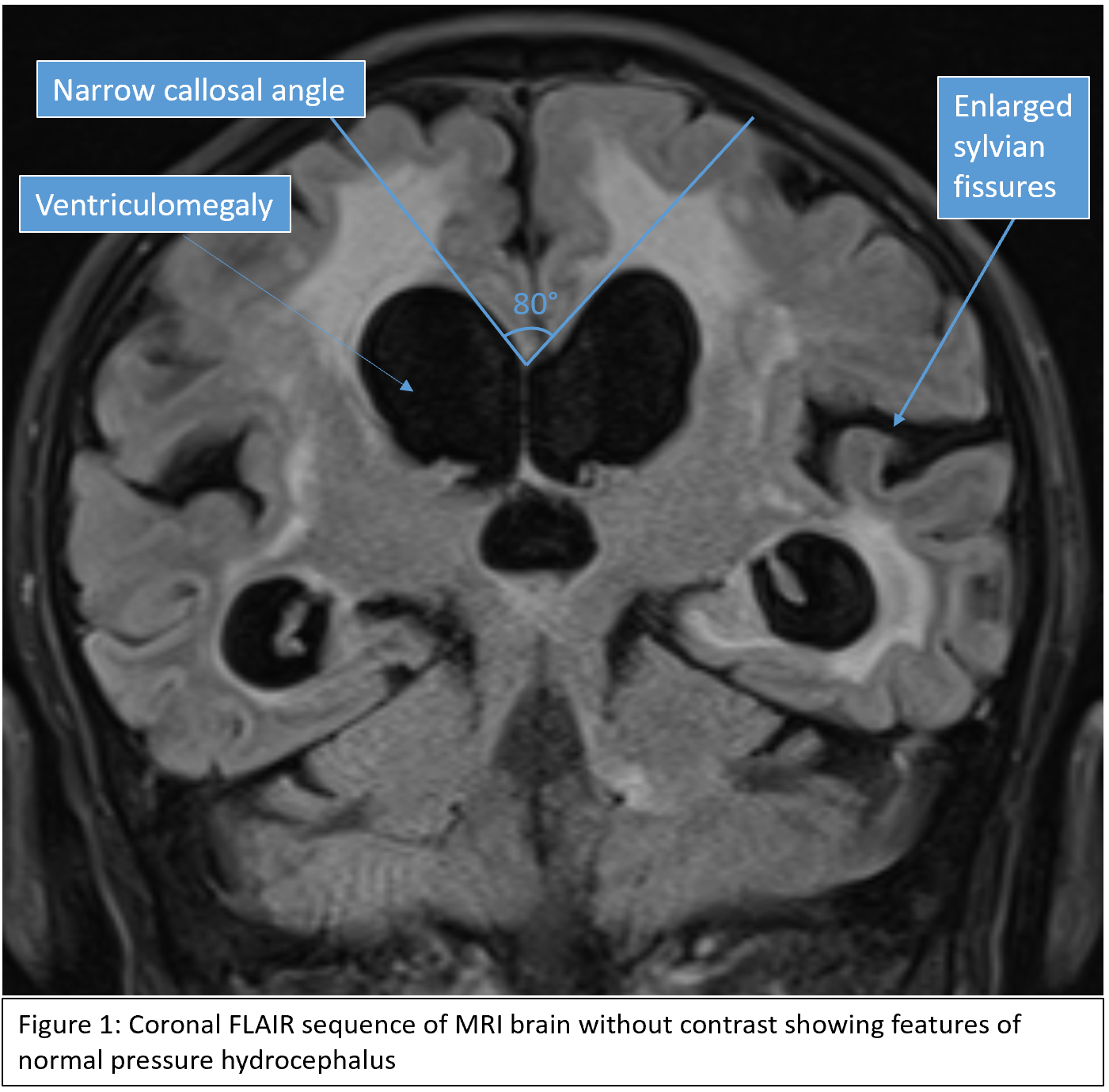
Background: Parkinsonism is characterised by bradykinesia, rigidity and rest tremor. Parkinsonism can arise from neurodegenerative and non-neurodegenerative conditions. Hydrocephalus is a structural condition that can cause parkinsonism, and is differentiated into obstructive or non-obstructive forms. Normal pressure hydrocephalus (NPH) is a progressive condition with a classic triad of gait disturbance, urinary incontinence and cognitive impairment. Patients with NPH can present with cardinal signs of Parkinson’s disease such as bradykinesia and rigidity.
Method: An 89-year-old previously well gentleman presented with a 1-week history of acute functional decline. A CT scan showed evidence of a metastatic lung malignancy. An MRI scan of the brain without contrast showed significant ventriculomegaly, and a diagnosis of normal pressure hydrocephalus was suggested. Further collateral history revealed a gradual decline over 4 months, with slowing of movement and ambulation. He later experienced frequent falls and developed cognitive decline and short-term memory loss. On examination, patient was found to be parkinsonian, with paucity of facial expression and soft voice. His limbs had increased tone bilaterally, with rigidity and bradykinesia worse on the left side. There was no tremor or cerebellar signs, and the patient exhibited normal muscle power and reflexes. Marked gait apraxia was present.
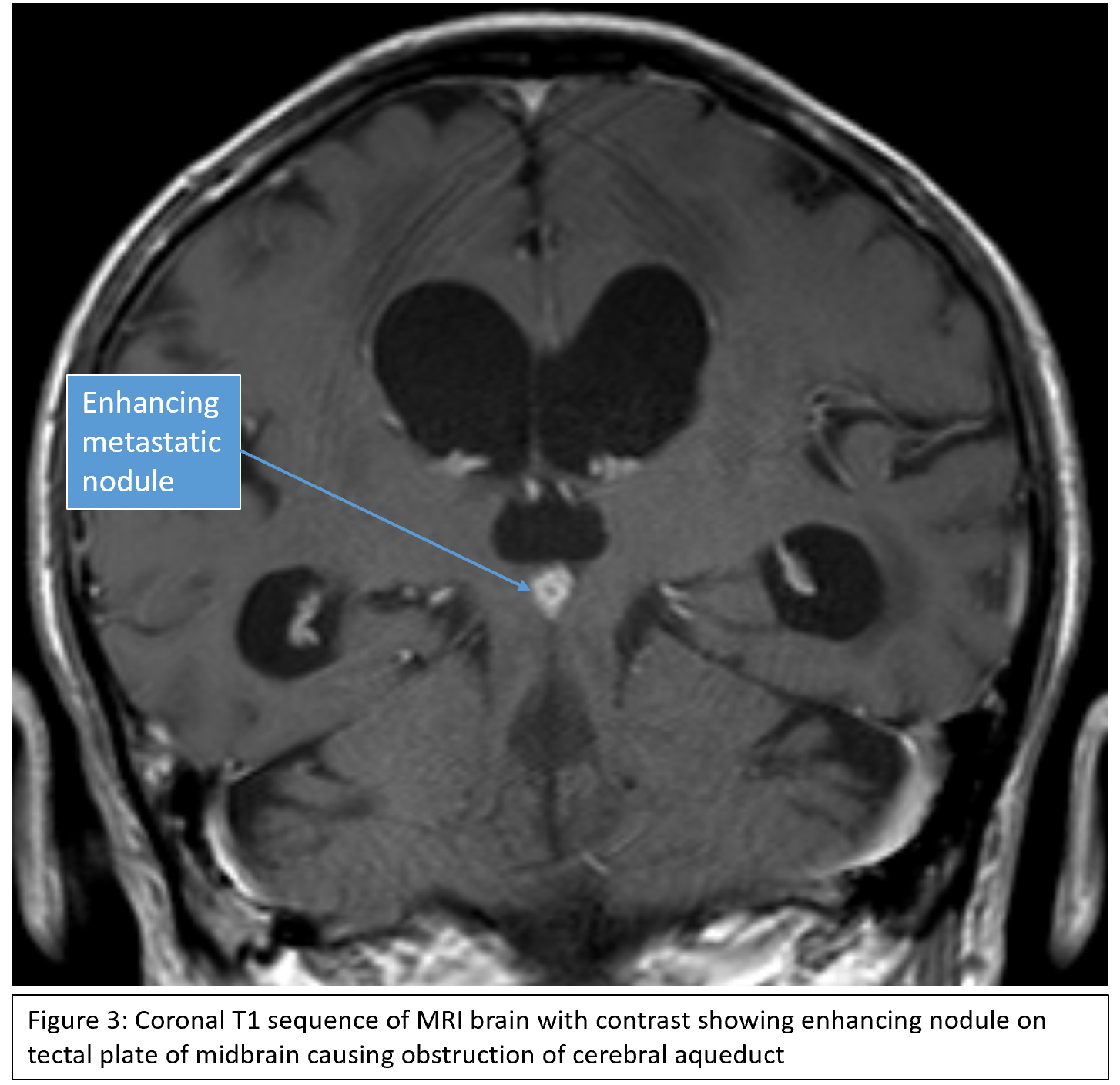
Results: The subacute development of parkinsonism in an elderly patient with malignancy was suspicious for a non-neurodegenerative cause. The rapid progression of clinical symptoms was atypical for a diagnosis of NPH. MRI brain with contrast showed multiple intracranial enhancing nodules representing metastatic deposits. Most notably a 0.7cm enhancing nodule at the tectal plate of the midbrain obstructed the cerebral aqueduct, resulting in obstructive hydrocephalus. Multidisciplinary care was initiated, and the patient’s family ultimately decided on palliative management with a focus on symptom control.
Conclusion: This case of obstructive hydrocephalus presenting as rapid onset parkinsonism reinforces the need for comprehensive history taking and interpretation of appropriate imaging sequences for accurate diagnosis.


References: 1. Saeed U, Lang AE, Masellis M. Neuroimaging advances in Parkinson’s disease and atypical Parkinsonian syndromes. Frontiers in Neurology. 2020 Oct 15;11:572976.
2. Bologna M, Truong D, Jankovic J. The etiopathogenetic and pathophysiological spectrum of parkinsonism. Journal of the Neurological Sciences. 2022 Feb 15;433:120012.
3. Aerts MB et al. Improving the diagnostic accuracy in parkinsonism: a three-pronged approach. Practical neurology. 2012 Apr 1;12(2):77-87.
4. Youn J et al. Parkinsonism and cerebrospinal fluid disorders. Journal of the Neurological Sciences. 2022 Feb 15;433:120019.
5. Ali K, Morris HR. Parkinson’s disease: chameleons and mimics. Practical neurology. 2015 Feb 1;15(1):14-25.
To cite this abstract in AMA style:
D. Tang, J. Vijayan, CH. Tan, SF. Woo, JH. Tan. Parkinsonism and dilated ventricles: not all hydrocephalus is normal-pressure [abstract]. Mov Disord. 2023; 38 (suppl 1). https://www.mdsabstracts.org/abstract/parkinsonism-and-dilated-ventricles-not-all-hydrocephalus-is-normal-pressure/. Accessed July 12, 2026.« Back to 2023 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/parkinsonism-and-dilated-ventricles-not-all-hydrocephalus-is-normal-pressure/