Category: Parkinson's Disease: Neurophysiology
Objective: Compare beta-power in the subthalamic nucleus (STN) between the most affected and least affected body side at disease onset.
Background: Exaggerated beta activity (13–35 Hz) throughout the basal ganglia is a widely replicated finding in Parkinson’s disease (PD)[1]. In addition the loss of dopaminergic transporter is lateralized and leads to an asymmetry in the severity of motor symptoms observed in most PD patients [2].
Method: Thirteen patients with PD treated with STN deep brain stimulation participated. Local field potentials (LFPs) from both STNs were recorded with the Medtronic Percept PC for 60 seconds of rest during both OFF and ON stimulation (mA based on individual clinically effective stimulation). The bipolar LFP time series of the contacts adjacent to the stimulating contact were used for further analyses. Power Spectral Densities (PSDs) were estimated between 1 and 125 Hz and normalized as percentage of total power. Spectral properties between both STNs (contralateral and ipsilateral to the most affected body-side at disease onset), were compared using cluster-based permutation testing [3]. Lead localization was determined using Lead DBS v3.0 [4,5]. Recordings took place ON dopaminergic medication.
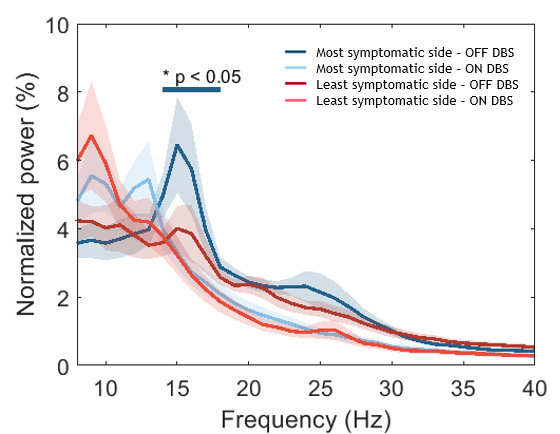
Results: In seven patients disease onset was on the right side. Mean (±SD) disease duration was 19.1±7.0 years and time since lead implantation was 6.6±1.3 years. At time of the recording, mean OFF-stimulation unilateral UPDRS scores (bradykinesia, rigidity and tremor items) were 12.6±5.9 for the most and 11.9±4.6 for the least affected body side at disease onset. There was a significant spectral difference between both sides in the OFF-stimulation condition involving the frequency range between 13 to 16 Hz (Figure 1). The beta peak frequencies were comparable between hemispheres. There was no relation between beta peak power and distance to the sensorimotor STN. The spectral difference between both hemispheres is not explained by differences in maximum beta power between different bipolar montages (either in “Streaming” or “Survey” mode).
Conclusion: Subthalamic LFP asymmetry in the low beta range is related to symptom asymmetry at disease onset, with a higher amplitude contralateral to the clinically more affected side at disease onset. This asymmetry in beta power is abolished during high-frequency stimulation.
References: 1. Brown 2007, doi: 10.1016/j.conb.2007.12.001.
2. Scherfler et al. 2012, doi: 10.1093/brain/aws253.
3. Maris et al. 2007, doi: 10.1016/j.jneumeth.2007.02.011.
4. Ewert et al. 2017, doi: 10.1016/j.neuroimage.2017.05.015.
5. Horn et al. 2015, doi: 10.1016/j.neuroimage.2014.12.002.
To cite this abstract in AMA style:
A. Buijink, F. Torrecillos, M. Stam, D. Piña-Fuentes, A. Pogosyan, C. Wiest, R. de Bie, P. Schuurman, G. Tinkhauser, H. Tan, M. Beudel. Parkinson’s disease symptom asymmetry at disease onset corresponds to low-beta power asymmetry in the subthalamic nucleus [abstract]. Mov Disord. 2022; 37 (suppl 2). https://www.mdsabstracts.org/abstract/parkinsons-disease-symptom-asymmetry-at-disease-onset-corresponds-to-low-beta-power-asymmetry-in-the-subthalamic-nucleus/. Accessed June 20, 2026.« Back to 2022 International Congress
MDS Abstracts - https://www.mdsabstracts.org/abstract/parkinsons-disease-symptom-asymmetry-at-disease-onset-corresponds-to-low-beta-power-asymmetry-in-the-subthalamic-nucleus/